- How It Works
- PhD thesis writing
- Master thesis writing
- Bachelor thesis writing
- Dissertation writing service
- Dissertation abstract writing
- Thesis proposal writing
- Thesis editing service
- Thesis proofreading service
- Thesis formatting service
- Coursework writing service
- Research paper writing service
- Architecture thesis writing
- Computer science thesis writing
- Engineering thesis writing
- History thesis writing
- MBA thesis writing
- Nursing dissertation writing
- Psychology dissertation writing
- Sociology thesis writing
- Statistics dissertation writing
- Buy dissertation online
- Write my dissertation
- Cheap thesis
- Cheap dissertation
- Custom dissertation
- Dissertation help
- Pay for thesis
- Pay for dissertation
- Senior thesis
- Write my thesis

180 Exercise Physiology Research Topics For Students

We know, you are reading this page because you are looking for the best and most interesting exercise physiology research topics one could possibly find on the Internet. After all, the grade you get on your next research paper depends a whole lot on the quality of the topic you manage to find. If you didn’t know, professors pay attention to what you are talking about.
If you manage to impress them right from the start by choosing an exceptional topic, they will usually give you some bonus points. It can really make the difference between a B and an A or even and A+. This is why we are proud to say that, on this page, you will find 180 unique, 100% original topics related to exercise psychology and kinesiology.
Getting The Best Exercise Physiology Research Topics
Many students don’t really pay attention to the topic they choose for their research papers. Unfortunately, they think that their writing skills alone are enough to convince their professor to give them an A+. As you might have guessed it already, this is not true. You can write an amazing paper on a boring topic (a topic that has been used by 3 other students in your class already) and still not get the coveted A+. So, here is why you should give our topics a try:
All of these topic ideas have been created by our professional academic writers. These people have been writing research papers for years, so they know what professors are looking for. Our exercise physiology research paper topics are not only very interesting to write about, they are also relatively easy. You can find plenty of information online about most of them. These topic ideas are 100 percent free. We want to help students get the top grades they need, which means we would never charge you for some great ideas. We are striving to update the list as frequently as possible. Why? Because we want to be able to help as many students as possible with unique topics for their exercise physiology research papers.
We know, you want to take a look at our exercise physiology research topics. Well, without further ado, here they are – organized neatly into relevant categories:
Kinesiology Research Topics
Are you looking for the absolute best kinesiology research topics on the Internet? Take a look at the list below and pick the topic you love right now:
- What is kinesiology and what does it do?
- The effects of physical activity on human cells
- The benefits of adapted physical activity for athletes
- Using physical activity to fight disease
- Arterial stiffness related to physical inactivity
- The effects of physical activity on neurons
Exercise Science Research Proposal Ideas
Do you need to write a research proposal about exercise science? Of course, we have a great list of exercise science research proposal ideas right here for you:
- Treatment of athletes’ knee joint injuries
- Health benefits of a whole-grain diet
- Healthy nutrition for athletes
- Physical exercises that alleviate autism symptoms
- Physical exercise for increasing bone density
- The effects of caffeine on physical exercise
- The dangers of sprains
- In-depth analysis of insulin levels in bodybuilders
- Outdoor physical activity for treating depression
- Preventing muscle fiber destruction during physical exercise
- The link between aggressiveness and physical exercise
- Exercise therapy as a treatment for osteoporosis
- Negative effects of intense bodybuilding training
Easy Exercise Science Research Topics
But what if you don’t want to spend too much time working on your exercise science paper? Then you simply pick one of the following easy exercise science research topics:
- The best exercises for abs
- The best exercises to get rid of belly fat
- The importance of warming up
- Exercises that work the biceps
- Excellent exercises for legs
- The latest breakthroughs in exercise science
- The workout routing for novice bodybuilders
- The best exercises for triceps
- Exercises that work the shoulders
- Targeting the chest during a workout
- Exercises for arms that you can do at home
- Exercises that target the glutes
- 3 methods to get a flat stomach in no time
- Latest research in exercise science
Exercise Physiology Topics Of Interest In 2023
If you want to talk about the latest advancements and research in exercise physiology, you need to take a look at our list of exercise physiology topics of interest in 2023:
- The role of exercise physiology in combating obesity
- The link between aerobic exercise and belly fat
- Compare aerobic and anaerobic physical exercises
- Using exercise physiology for heart rehabilitation
- Can exercise physiology find a cure for diabetes?
- Analyze the body’s ability to adapt to difficult physical activity
Kinesiology Topics Your Professor Will Love
In case you want a topic that you are guaranteed to be appreciated by your professor, you should definitely pick one of the kinesiology topics your professor will love:
- Is kinesiology a good career?
- What I find most interesting about kinesiology
- Using kinesiology to find underlying causes of health problems
- Applications of kinesiology in modern medicine
- Kinesiology applications used by top athletes today
- Discuss the 3 major principles of kinesiology
Fitness Research Paper Topics
Why wouldn’t you talk about fitness? There is nothing wrong about it because it is a part of physical exercise research. In fact, here are a few great fitness research paper topics:
- Effects of Zumba on the human body
- Discuss cross fit training
- The benefits of stretching before a workout
- Analyze the benefits of circuit training
- Is bike riding an effective exercise?
- Pilates: effects on the body
- Benefits of taking spinning classes
- Discuss the way HIIT workouts work
- Talk about plyometric exercises
- Best routines for strength training
- Running and its health benefits
- Is yoga a form of physical exercise?
University Level Topics
Be aware that university level topics are not as easy to write about. If you want to try writing such a paper, check out the university level topics below:
- Psychological principles in kinesiology
- Discuss applied kinesiology in 2023
- The biomechanics of the human wrist
- Kinesiology applications in developing prosthetics
- Developing a diet and workout plan for a bodybuilder from scratch
Controversial Exercise Physiology Topics
There is nothing that could prevent you from writing about a controversial idea. Your professor will love these controversial exercise physiology topics:
- Depression and suicide rates in young athletes in the United States
- Anxiety and stress caused by extreme physical exercise
- Sleep disorders caused by physical exercise
- Who can afford expert exercise physiology advice?
- The most controversial exercise physiology papers ever published
Topics That Received High Grades
In our experience, some topics received better grades than others. Here are the topics that received high grades. Give them a try:
- The best fitness trackers in 2023
- The beginner’s guide to meal planning
- The correct ratio of fat, carbs and protein
- Healthy diets in United States schools
- A detailed explanation of muscle contraction
- Making muscle fibers grown
- Effects of physical activity on the nervous system
- Conditions that can be cured with physical exercise
- Discuss the process of healing fractures
- Effects of physical fitness training dangerous on stroke patients
- Changes in physical performance of the elderly over the last 50 years in the UK
- Discuss the pros and cons of the Paleo diet
- Calculating the amount of protein for bodybuilder meals
- Movement patterns that lead to injuries
- The link between physical exercise and a correct posture
Physical Exercise And Health Topics
Want to talk about how physical exercise affects the human health? No problem! Take a look at some of the best physical exercise and health topics for 2023 and possibly even 2024:
- The link between physical activity and academic performance
- Physical exercise can boost the immune system
- Study the physical activity of college students
- The role of physical exercise in a healthy diet
- Effects of HIIT exercises on health
- Cardiovascular health and physical exercise
- Can physical activity prevent diabetes?
Exercise Science Topics For High School
Are you a high school student? Do you need to write an exercise science academic paper? Then you should definitely take a look at these exercise science topics for high school:
- Positive effects of sports video games
- Is running good or bad for our health?
- Ways to deal with stress as an athlete
- Things that can affect sports performance
- Effects of barefoot running
- Negative effects of prolonged high-intensity interval training exercises
- Compare and contrast 3 different popular diets
- Preventing sports-related injuries in high schools
- Why are some people more flexible?
- Discuss the term “neuroplasticity”
- Talk about the psychological effects of physical exercise
- How do bones develop?
- The role of the skeleton in maintaining balance
- Can physical exercise make us better people?
Difficult Kinesiology Topics For High School
But what if you want to write about a more difficult topic? We’ve got you covered. Check out our list of difficult kinesiology topics for high school:
- Discuss the 3 main principles of kinesiology
- The neuroplasticity principle in kinesiology
- The role of kinesiology in biomechanics
- The adaptation through exercise principle
- Training elite athletes using the principles of kinesiology
- And in-depth look at the motor redundancy principle
- Kinesiology research for developing orthopedics
- Applications of kinesiology in sport psychology
- Latest research breakthroughs in kinesiology
- Is kinesiology a regulated health profession?
- Using kinesiology to rehabilitate workplace injuries
- Kinesiology in long-term care applications
- Benefits of kinesiology for athletes
Health And Fitness Research Topics
Interested about health and fitness? No list would be complete without some exceptional health and fitness research topics, we know. Pick any of these right now:
- The 10 best exercises to try at home
- Best cardio exercise for home
- Improve your fitness and your health
- Documenting one-s fitness journey
- Pros and cons of sports supplements
- The effects of vitamins on your workout
- A healthy fitness goal
- Benefits of fitness trackers
- Discuss the 3 main health benefits of fitness
- The best health-focused training plan
- Workouts that help people with depression
- Negative effects of HIIT on health
- 3 reasons to avoid physical exercise
- Doing workouts and preventing injury
- The importance of the shoes you wear during workouts
Physical Activity Research Topics
If you want to write about physical activity, then you should definitely choose one of our relatively simple physical activity research topics:
- Effects of brisk walking on the human body
- The main benefits of jogging
- The biomechanics behind weight lifting exercises
- Effects of alcohol on physical activity
- Physical activity can prevent colds and the flu
- Discuss the link between physical inactivity and noncommunicable diseases
- Difference between walking uphill and downhill
Interesting Topics In Exercise Physiology
Our experienced writers and editors managed to compile a list of the most interesting topics in exercise physiology just for you:
- The tech behind body composition testing
- Talk about elevation training
- Interesting hearth rate variability research
- What is the maximal aerobic speed?
- Talk about the concept of neuroplasticity
- Effects physical exercise on cardiovascular health
- Effects of nutrition on your workouts
Physical Exercise And Mental Health Topics
Yes, physical exercise really does affect mental health. Here are some very nice physical exercise and mental health ideas that you can write about right now:
- How does physical exercise affect your mental health?
- Exercises that reduce depression
- Why is daily exercise so important?
- Physical signs that you are dealing with stress
- Exercises that reduce anxiety
- Exercises that improve your mood
- Physical exercises for autistic children
Physiology Research Topics For College Students
College students who want to write a research paper about physiology should choose one of these unique physiology research topics for college students:
- Talk about motor teaching in kinesiology
- Pick a muscle and analyze its anatomy
- Analyze the biomechanics of the hip
- Discuss motor learning in kinesiology
- An in-depth look a muscle synergies
- Analyze the biomechanics of the intervertebral joints
- Gait pattern changes during the human life
Sport Science Research Topics
Interested in some nice sport science research topics that should make writing your academic paper easier? Here is a list of the best ones, just for you:
- Best ways to monitor the onset of fatigue
- Discuss the role of wearables in sport science
- What does sport science do?
- An in-depth look at hydration testing
- Monitoring the growth of muscles after exercise
- Discuss the process of bio-banding
- Differences between technical, chronological and biological age
Interesting Topics About Kinesiology
Finally, we have a list of the most interesting topics about kinesiology we could think of. Again, all these ideas are original, so don’t hesitate to snatch one right now:
- Athletes that became famous with help from kinesiology
- Muscle activation during simple movements
- Talk about exercises that increase endurance
- Maintaining correct posture during workouts
- The biomechanics of running
- Discuss about the composition of human bones
- An in-depth look at muscular contractions
- Best exercises for strength
- Best 3 ways to make your muscles grow
- The role of the skeleton
- Talk about the different types of muscles
- Discuss the join structure of humans
- Exercises that increase flexibility
- The biomechanics of lifting exercises
Get Top-Notch Research Paper Writing Service
If you want to get a top grade on your next exercise physiology research paper, you should seriously consider getting our help. We are the best and most affordable top-notch research paper writing service on the Internet. The truth is that we have been writing academic essays for students of all ages for over 10 years.
Getting writing help is now easier than ever. High school, college and university students can simply get in touch with us and tell us what they need. We will immediately assign one of our professional, ENL writers to their academic paper. All our expert writers have PhD degrees in various fields, including exercise physiology/kinesiology. WE are your best option for getting a top quality custom essay fast and cheap online. Get in touch with our 24/7 customer support and let’s get started on your next awesome research paper!

Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Comment * Error message
Name * Error message
Email * Error message
Save my name, email, and website in this browser for the next time I comment.
As Putin continues killing civilians, bombing kindergartens, and threatening WWIII, Ukraine fights for the world's peaceful future.
Ukraine Live Updates
Explore your training options in 10 minutes Get Started
- Graduate Stories
- Partner Spotlights
- Bootcamp Prep
- Bootcamp Admissions
- University Bootcamps
- Coding Tools
- Software Engineering
- Web Development
- Data Science
- Tech Guides
- Tech Resources
- Career Advice
- Online Learning
- Internships
- Apprenticeships
- Tech Salaries
- Associate Degree
- Bachelor's Degree
- Master's Degree
- University Admissions
- Best Schools
- Certifications
- Bootcamp Financing
- Higher Ed Financing
- Scholarships
- Financial Aid
- Best Coding Bootcamps
- Best Online Bootcamps
- Best Web Design Bootcamps
- Best Data Science Bootcamps
- Best Technology Sales Bootcamps
- Best Data Analytics Bootcamps
- Best Cybersecurity Bootcamps
- Best Digital Marketing Bootcamps
- Los Angeles
- San Francisco
- Browse All Locations
- Digital Marketing
- Machine Learning
- See All Subjects
- Bootcamps 101
- Full-Stack Development
- Career Changes
- View all Career Discussions
- Mobile App Development
- Cybersecurity
- Product Management
- UX/UI Design
- What is a Coding Bootcamp?
- Are Coding Bootcamps Worth It?
- How to Choose a Coding Bootcamp
- Best Online Coding Bootcamps and Courses
- Best Free Bootcamps and Coding Training
- Coding Bootcamp vs. Community College
- Coding Bootcamp vs. Self-Learning
- Bootcamps vs. Certifications: Compared
- What Is a Coding Bootcamp Job Guarantee?
- How to Pay for Coding Bootcamp
- Ultimate Guide to Coding Bootcamp Loans
- Best Coding Bootcamp Scholarships and Grants
- Education Stipends for Coding Bootcamps
- Get Your Coding Bootcamp Sponsored by Your Employer
- GI Bill and Coding Bootcamps
- Tech Intevriews
- Our Enterprise Solution
- Connect With Us
- Publication
- Reskill America
- Partner With Us
- Resource Center
- Bachelor’s Degree
- Master’s Degree
The Top 10 Most Interesting Exercise Science Research Topics
The field of exercise science is rapidly growing as new technologies like computer visualization and biotracking deepen our understanding of human physiology. New technologies allow us to better prevent injuries, allowing athletes to push their limits beyond what we thought possible. Thanks to this, there is no shortage of exercise science research topics to write about.
In this article, we’ll show you 10 great examples of exercise science research topics. If you are pursuing a degree in this field, you’ll learn better ways of finding good exercise science research paper topics and how to develop stronger exercise science research questions for your projects.
Find your bootcamp match
What makes a strong exercise science research topic.
Strong exercise science research topics are timely and relevant. Leading researchers and sports institutions should still be discussing them at the time you are writing your research paper. The Strength and Conditioning Journal is a great place to find some of the latest activity research topics including articles on different health benefits, health issues, preventive interventions, and rehabilitation after injury.
Your topic should be broad enough to find enough strong sources, but narrow enough to stand out. Controversial topics are acceptable if you have enough evidence to back up your research. If it’s your first paper, consider approaching a less complex topic. You can also ask your teacher for suggestions if you are struggling to find strong university-level topics. Remember to follow the guidelines for choosing a topic set by your institution.
Tips for Choosing an Exercise Science Research Topic
- Choose a topic that intrigues you. A personally interesting topic will motivate you during the research process. If you have a personal connection to what you are researching, you will have a much easier time writing about it.
- Narrow your topic. By picking a specific subject, you will have an easier time finding credible sources to support your research. By reducing the number of books and articles to read and only choosing literature that is immediately relevant to your topic idea, you also won’t have to spend as much effort before starting to write.
- Talk to your teacher or academic advisor. Your teachers are great resources you have at your disposal. They have experience choosing topics for college students and will most likely be able to help you pick a topic you’ll find engaging to research.
- Look through journals to find exciting topics. Review topics published in the journals like the Journal of Strength and Conditioning Research. These research journals publish the latest fitness research papers and can help you find a topic that interests you.
- Consider the research interests of your teacher. It’ll be convenient if your research topic matches their expertise, as they’ll be able to provide you with better feedback during your research process.
What’s the Difference Between a Research Topic and a Research Question?
A research topic is a specific area of study. Sprains in adult athletes or rehabilitation for brain injuries, for example, are research topics. A research question is a way to add new knowledge to that area of study. Examples of research questions would be “What is the role of nutrition in the recovery of sprains in athletes?” or “What is the effect of cardio exercises on adults with brain injuries?”
The goal of your research should be focused around answering the research question. Your answer will help you and others to understand the topic better. Research questions tend to be more specific than the research topics in exercise science.
How to Create Strong Exercise Science Research Questions
To create strong exercise science research questions, you should first become familiar with the topic the question concerns. The answer to your research question should be supported by previous studies done on the topic. Reading previously published studies will help you learn more while preventing you from doing any redundant research.
The scientific method helps exercise scientists better understand their field. Your question should start with how, why, when, or what questions. The scope of your question must be manageable in relation to how long you have to answer it.
Questions that require in-depth experiments may be beyond your reach if you only have a week. Before choosing the question that will lead your research, consider the time it will take you to answer it.
Top 10 Exercise Science Research Paper Topics
1. benefits of resistance training for reducing the negative consequences of aging.
Metabolic resistance training can counter the adverse effects of aging. According to a 2019 study by the Journal of Strength and Conditioning Research, only nine percent of older adults in the United States practice any form of resistance or weight lifting exercises. Metabolic resistance training for elderly residents has become a recently popular topic, as it has been proven to increase muscle mass and muscle strength and relieve intervertebral joint pain.
2. Determining the Minimal Amount of Physical Exercise Required to Maintain Strength and Stamina
Long periods of physical inactivity harm physical fitness. Scientists want to know how much physical exercise can prevent the loss of muscle strength. The British Journal of Sports Medicine published an article that took an in-depth look into the negative effects of sedentary behavior . There are plenty of physiology research topics about improving daily life with an active lifestyle.
3. Effect of a Low-Carbohydrate Ketogenic Diet on Body Mass on Olympic Weightlifting Athletes
Exercise scientists have realized the impact of nutrition on endurance, body composition, and recovery. This has led to theories being tested of controversial ideas in nutrition and measuring their effects on muscle strength.
For example, a study by the Journal of Strength and Conditioning Research shows that ketogenic diets reduce mass without compromising performance . If you are interested in becoming a nutritionist , researching the role of nutrition in relation to physical activity could be beneficial for your future career.
4. The Effect of Exercise on the Gut Microbiome
The role of exercise on the gut microbiome is an exciting topic in exercise science. In 2019, researchers found some proof that regular exercise increased gut bacteria and contributed to the health of the gut microbiome, as mentioned in a study that was published in Exercises and Sport Science Reviews.
The gut microbiome produces a wide range of biomolecules, including neurotransmitters, that regulate mood and anxiety. Researchers believe that healthy gut bacteria can improve our mental fitness and health. Their research also leads them to believe that gut bacteria can improve the body’s ability to fight inflammatory illnesses and certain types of cancer.
5. Wearable Technology for Health Monitoring and Sport Performance
Smartwatches pack sensors that can track your movement patterns, heart rate, and oxygen levels. In recent years, these bio trackers have become increasingly affordable and easy to use. Researchers at the School of Kinesiology at the University of Michigan have used these sensors to track elderly patients and alert their caregivers in real-time.
In sports, kinesiologists use this technology to measure aerobic speed and the onset of fatigue. With a degree in kinesiology , you can work with elite athletes and improve their athletic performance using these technologies.
6. Optimizing Human Movement Potential for Elite Athletes
Exercise scientists study the biomechanics of human movement to improve the body’s longevity. Understanding the human body allows researchers to develop primary injury prevention methods.
Personal trainers help athletes achieve extraordinary performance without the risk of musculoskeletal injury. If you want to become a certified personal trainer , physiology research paper topics in relation to this topic may be of interest to you.
7. Equity in Sports
Exercise scientists are also concerned with the social aspects of sports. Many athletes live under adverse conditions and need to make extra efforts to match the achievements of others. Equity in sports is currently a very important exercise science topic. Researchers find solutions to increase access to professional sports by improving policies to prevent racism, sexism, and other forms of discrimination.
If you want to become a sports agent or an athletic director, look for physiology research topics in relation to equity in sports. Becoming a sports manager takes a certain level of education in the professional fitness industry, such as a graduate degree in sports management .
8. Effect of Bike Commuting on Insulin Sensitivity, Cardiorespiratory Fitness, and Adipose Tissue
Exercise scientists look for solutions to public health problems like diabetes and obesity. A study published in the British Journal of Sports Medicine found that commuting by bike has a significant impact on insulin sensitivity , improving cardiovascular fitness, and reducing belly fat.
With cardiometabolic health such as cardiovascular disease, being an urgent topic in the United States, considering the prevalence of obesity, there is plenty of research on the subject, making it a great initial topic.
9. Reducing Lower Back Pain by Increasing Physical Activity
With athletes having a high sports injury risk, and many injuries causing severe back pain, pain management has become an important topic in exercise science. Exercise scientists research ways to reduce pain using principles in kinesiology and found that increasing physical activity can reduce lower back pain , according to a study published in the British Journal of Sports Medicine.
10. Applications of Kinesiology in the Treatment of Movement Dysfunctions
Exercise scientists have been studying the relationship between movement and neuroplasticity for a long time. Physical activity during rehabilitation for stroke patients or patients with brain injuries has proven to reduce movement dysfunctions. Understanding the effects of exercise on neural networks is an important research topic in the field of rehabilitation.
Other Examples of Exercise Science Research Topics & Questions
Exercise science research topics.
- Assessment of the use of virtual reality rehabilitating brain-injured or stroke patients
- The role of caffeine as a sports performance enhancer for optimal performance
- Current and future perspectives on the effects of nutrition on physical exercise performance
- Hormonal responses in older men to metabolic resistance training
- Comparison of occupational physical activity and leisure physical activity on cardiovascular fitness
Exercise Science Research Questions
- What are the benefits of physical activity for cognitive health?
- What is the impact of VR training on human body composition testing?
- What are the advantages of wearing an elevation training mask during physical exercise?
- What are the physiological causes of mental fatigue on endurance performance?
- How does physical exercise improves mental health and academic performance in university students?
Choosing the Right Exercise Science Research Topic
When choosing the right exercise science research topic, consider researching topics that you are already familiar with, as your existing knowledge may help you with your research. You could also ask your academic advisor, other staff in the department of exercise science, or even physical therapy professionals about current trends in exercise science and injury recovery.
Physical fitness and training performance are common themes in exercise science research. Recent articles published by the British Journal of Sports Medicine or the Journal of Strength and Conditioning Research are a great place to start. Make sure you choose a manageable research topic. Your teacher can help you make sure your research topic is relevant before you begin.

"Career Karma entered my life when I needed it most and quickly helped me match with a bootcamp. Two months after graduating, I found my dream job that aligned with my values and goals in life!"
Venus, Software Engineer at Rockbot
Exercise Science Research Topics FAQ
Exercise science is important because it tries to find solutions to problems concerning the optimal performance of athletes and the general health of the human population. Exercise science also helps develop new rehabilitation methods for injury recovery and pain management.
Yes, kinesiology is a STEM discipline that studies exercise and movement. Breakthroughs in kinesiology come from scientific research and the use of the scientific method. It is a wing of the department of exercise science of many universities.
The average salary of an exercise physiologist is $50,280 per year, which is above the national average, according to the Bureau of Labor Statistics. About half of all exercise physiologists are self-employed, while others work in hospitals, spas, and physical therapy offices.
With a Bachelor’s Degree in Exercise Science, you can get a job as a physical therapist or a fitness instructor. With a graduate degree in exercise science, you can become a sports agent or an athletic director.
About us: Career Karma is a platform designed to help job seekers find, research, and connect with job training programs to advance their careers. Learn about the CK publication .
What's Next?
Get matched with top bootcamps
Ask a question to our community, take our careers quiz.

Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *

Physical Fitness Research Paper Topics

Looking for captivating physical fitness research paper topics ? You’ve come to the right place! This page is your ultimate resource, providing an extensive list of research paper topics that delve into the fascinating world of physical fitness. With ten categories, each containing ten unique physical fitness research paper topics, you’ll discover a wide range of subjects to explore, analyze, and present in your research. From exercise physiology to nutrition, psychology to biomechanics, this comprehensive list covers various dimensions of physical fitness. So, whether you’re passionate about understanding the effects of exercise on cardiovascular health or exploring the role of nutrition in athletic performance, these topics will ignite your curiosity and help you embark on a rewarding research journey in the realm of physical fitness.
100 Physical Fitness Research Paper Topics
The field of physical fitness offers a rich landscape for research, providing numerous opportunities for students to explore various aspects of human health, exercise, and performance. This comprehensive list of physical fitness research paper topics is designed to inspire and guide health science students in their quest for compelling research ideas. The list is divided into ten categories, each containing ten unique topics, offering a diverse range of subjects to delve into. Whether you are interested in the physiological, psychological, or social aspects of physical fitness, there is something for everyone in this extensive compilation.
Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% off with 24start discount code.
Exercise Physiology
- The impact of different exercise modalities on cardiovascular health.
- Effects of resistance training on muscle strength and hypertrophy.
- The role of aerobic exercise in improving cognitive function.
- Exploring the physiological mechanisms behind exercise-induced fatigue.
- Exercise and its impact on metabolic disorders such as diabetes.
- The influence of exercise on bone health and prevention of osteoporosis.
- Effects of high-intensity interval training (HIIT) on athletic performance.
- The relationship between exercise and immune function.
- Exploring the effects of exercise on sleep quality and duration.
- The impact of exercise on mental health and well-being.
Nutrition and Physical Fitness
- The role of macronutrients in optimizing athletic performance.
- Exploring the effects of different diets on body composition and fitness.
- The influence of nutritional supplements on exercise recovery and performance.
- The impact of hydration status on exercise performance and physiological responses.
- Nutritional strategies for optimizing muscle glycogen storage and utilization.
- Exploring the relationship between nutrition, gut microbiota, and physical fitness.
- The effects of fasting and intermittent fasting on exercise adaptations.
- Nutritional considerations for vegan and vegetarian athletes.
- The role of antioxidants in mitigating exercise-induced oxidative stress.
- Investigating the effects of pre- and post-exercise nutrition timing on performance and recovery.
Psychology of Exercise
- The psychological benefits of physical activity on stress reduction.
- Exploring the motivational factors influencing exercise adherence.
- The role of exercise in improving body image and self-esteem.
- Examining the relationship between exercise and cognitive function in older adults.
- The impact of exercise on mood disorders such as depression and anxiety.
- Investigating the psychological effects of team sports participation.
- Exploring the psychological strategies for enhancing exercise performance.
- The influence of exercise on cognitive and academic performance in students.
- The role of exercise in promoting healthy aging and cognitive longevity.
- Psychological factors influencing exercise behavior among different populations.
Biomechanics and Kinetics
- Investigating the biomechanics of human gait and its implications for injury prevention.
- The role of biomechanical analysis in optimizing sports performance.
- Understanding the mechanics of resistance training exercises for muscle activation.
- Examining the biomechanical factors influencing running economy and performance.
- Biomechanical analysis of joint loading during different types of exercise.
- The influence of footwear on biomechanics and injury risk in athletes.
- Exploring the mechanics of human balance and stability during exercise.
- The role of motion capture technology in studying human movement patterns.
- Biomechanical analysis of sports-specific movements and injury prevention.
- Investigating the mechanics of plyometric training and its impact on power development.
Sports Medicine and Injury Prevention
- Exploring the most common sports-related injuries and their prevention strategies.
- The role of rehabilitation and physical therapy in sports injury recovery.
- Investigating the effects of preventive measures on reducing concussion risk in contact sports.
- Understanding the biomechanics of common overuse injuries in athletes.
- Exploring the psychological factors influencing injury rehabilitation and return to sport.
- The impact of sports specialization on injury risk and long-term athlete development.
- Investigating the efficacy of different injury prevention programs in specific sports.
- The role of bracing and protective equipment in injury prevention.
- Exploring the influence of environmental factors on injury risk in outdoor sports.
- The effects of fatigue on injury occurrence and prevention in sports.
Physical Fitness Assessment and Testing
- Evaluating the validity and reliability of different fitness assessment methods.
- The role of body composition analysis in assessing physical fitness and health.
- Investigating the accuracy of wearable fitness trackers in monitoring exercise intensity.
- Examining the utility of field-based fitness tests in predicting athletic performance.
- Comparing the effectiveness of laboratory-based and field-based fitness assessments.
- Exploring novel approaches to assessing muscular strength and power.
- The role of cardiovascular fitness testing in predicting health outcomes.
- Investigating the assessment of flexibility and its relationship with injury risk.
- Examining the utility of functional movement screening in assessing physical fitness.
- Evaluating the psychometric properties of self-report physical activity questionnaires.
Exercise Prescription and Training Programs
- The effects of different exercise intensity and duration on fitness outcomes.
- Investigating the impact of periodization models on long-term athletic development.
- Optimizing resistance training program design for muscle hypertrophy.
- The role of concurrent training in maximizing strength and endurance gains.
- Exploring the benefits of high-intensity interval training (HIIT) in various populations.
- Examining the effects of different exercise modalities on body composition changes.
- Investigating the efficacy of exercise programs for older adults in improving functional capacity.
- The impact of exercise programming on cardiovascular health and disease prevention.
- Exploring the effects of exercise on insulin sensitivity and metabolic health.
- The role of exercise prescription in promoting weight loss and weight management.
Exercise and Special Populations
- Investigating the effects of exercise on pregnancy outcomes and maternal health.
- Exercise interventions for individuals with chronic diseases such as diabetes and cardiovascular disorders.
- The impact of exercise on bone health in postmenopausal women.
- Exploring exercise programs for individuals with physical disabilities.
- The role of exercise in managing symptoms and improving quality of life in cancer patients.
- Exercise interventions for individuals with mental health conditions such as depression and anxiety.
- Investigating the effects of exercise on cognitive function in children and adolescents.
- The impact of exercise on sleep quality and patterns in different populations.
- Exercise programs for older adults to enhance mobility, balance, and functional independence.
- The role of exercise in promoting well-being and reducing stress in the workplace.
Exercise and Public Health
- Investigating the impact of physical activity interventions on population health outcomes.
- The role of exercise in preventing and managing non-communicable diseases.
- Examining the socioeconomic factors influencing physical activity levels in different populations.
- Exploring the effectiveness of community-based exercise programs in promoting health.
- The impact of built environment and neighborhood design on physical activity levels.
- Investigating the relationship between physical fitness and academic performance in school settings.
- Exploring strategies to promote physical activity in sedentary populations.
- The role of exercise in reducing healthcare costs and burden on the healthcare system.
- Investigating the effects of policy and environmental changes on physical activity promotion.
- The role of exercise in promoting healthy aging and preventing age-related chronic diseases.
Emerging Trends and Innovations in Physical Fitness
- Investigating the effects of wearable technology on exercise motivation and behavior change.
- Exploring the potential of virtual reality in enhancing exercise experiences.
- The impact of exergaming on physical activity levels and health outcomes.
- Investigating the use of artificial intelligence in personalized exercise prescription.
- Exploring the effects of biofeedback techniques on performance and exercise adherence.
- The role of genomics in understanding individual responses to exercise.
- Investigating the effects of mind-body exercise modalities on physical and mental well-being.
- Exploring the potential of outdoor adventure and nature-based activities in promoting physical fitness.
- The impact of social media and online platforms on exercise motivation and support.
- Investigating the effects of environmental factors on exercise performance and adherence.
This comprehensive list of physical fitness research paper topics offers a vast array of possibilities for students to explore in their research endeavors. From exercise physiology to sports medicine, psychology to emerging trends, there are numerous avenues to delve into the fascinating field of physical fitness. Whether you have a specific interest in a particular category or wish to explore cross-disciplinary topics, this list provides a solid foundation for selecting a compelling research topic. So, let your curiosity guide you, and embark on a journey of discovery and knowledge in the realm of physical fitness research.
Physical Fitness: Exploring the Range of Research Paper Topics
Physical fitness is a multidimensional concept that encompasses various aspects of health, performance, and well-being. As a student of health sciences, delving into the realm of physical fitness research can provide you with a rich opportunity to explore a wide range of captivating topics. From understanding the physiological adaptations to exercise to investigating the psychological aspects of physical activity, the field of physical fitness offers an expansive landscape for research. In this article, we will explore the diverse range of physical fitness research paper topics, providing you with a comprehensive understanding of the exciting possibilities that lie ahead.
Exercise Physiology: Unraveling the Mysteries of Human Performance
Exercise physiology is a fundamental area of study within physical fitness research. It focuses on understanding how the body responds and adapts to exercise. One fascinating research area within exercise physiology is the investigation of physiological adaptations to different types of exercise. You can explore the effects of various exercise modalities, such as aerobic training, resistance training, or high-intensity interval training, on cardiovascular health, muscular strength, endurance, and body composition. Additionally, examining the impact of exercise on metabolic disorders, bone health, immune function, and fatigue can provide valuable insights into the physiological mechanisms underlying human performance.
Psychology of Physical Activity: Understanding the Mind-Body Connection
Understanding the psychological aspects of physical activity is crucial for promoting and maintaining engagement in exercise. The psychology of physical activity encompasses a broad range of physical fitness research paper topics that explore the factors influencing exercise motivation, adherence, and the interplay between physical activity and mental health. You can investigate the role of motivation in initiating and sustaining exercise behavior, exploring strategies to enhance exercise adherence and overcome barriers to physical activity participation. Furthermore, exploring the relationship between exercise and mental health outcomes, such as depression, anxiety, stress management, and cognitive function, can shed light on the potential psychological benefits of physical fitness.
Sports Nutrition: Fueling the Body for Optimal Performance
Nutrition plays a critical role in supporting physical fitness and performance. Researching the impact of nutrition on exercise performance and recovery is a dynamic field within the realm of physical fitness. You can explore topics such as the influence of macronutrient composition on endurance or strength performance, the effects of hydration on exercise capacity, the role of dietary supplements in enhancing athletic performance, and the timing and composition of pre- and post-exercise meals. Investigating the nutritional requirements of specific populations, such as athletes, older adults, or individuals with chronic diseases, can provide valuable insights into optimizing nutrition strategies for diverse populations.
Injury Prevention and Rehabilitation: Ensuring Safe and Effective Exercise
Injury prevention and rehabilitation are essential components of physical fitness research. Exploring topics related to injury prevention and rehabilitation can encompass a wide range of areas, including the identification of risk factors for exercise-related injuries, the development of effective training programs to reduce injury rates, the investigation of rehabilitation techniques to facilitate recovery and return to physical activity, and the evaluation of preventive strategies in specific populations. Understanding the mechanisms underlying injuries and developing strategies to mitigate their occurrence can contribute to safer and more effective exercise practices.
Exercise Prescription and Programming: Tailoring Fitness Interventions
Exercise prescription and programming focus on the design and implementation of exercise interventions tailored to individual needs and goals. This research area encompasses topics such as the development of personalized exercise programs for different populations, the optimization of training variables (intensity, duration, frequency) for specific outcomes, the evaluation of novel training methods and technologies, and the use of wearable devices and digital technologies in exercise prescription. Investigating exercise prescription and programming can provide valuable insights into the most effective strategies for achieving desired fitness outcomes, improving overall health and well-being, and promoting behavior change.
Biomechanics and Movement Analysis: Exploring Human Motion
Biomechanics and movement analysis involve the study of human motion and the forces that act upon the body during physical activities. This research area explores topics such as the mechanics of joint movement, muscle function, gait analysis, balance and coordination, and the effects of external factors on movement performance. Investigating biomechanics and movement analysis can contribute to a deeper understanding of optimal movement patterns, injury mechanisms, ergonomics, and the development of assistive devices or rehabilitation strategies.
Environmental and Occupational Health: Exploring the Impact of Work and Environment on Health
Environmental and occupational health focuses on the effects of work and environmental factors on human health and well-being. This research area encompasses topics such as the impact of physical activity in occupational settings, the effects of environmental pollutants on health outcomes, the role of physical fitness in occupational performance, and the development of strategies to promote a healthy work environment. Investigating environmental and occupational health can provide insights into the relationship between physical fitness, work-related factors, and overall health and safety.
Public Health and Health Promotion: Advancing Population Health
Public health and health promotion research aim to improve the health and well-being of populations through disease prevention, health education, and promotion of healthy behaviors. This research area explores topics such as the impact of physical fitness on chronic disease prevention, the effectiveness of health promotion interventions in promoting physical activity, strategies for increasing physical activity in underserved populations, and the development of policies to support physical fitness initiatives. Investigating public health and health promotion can contribute to the development of evidence-based interventions and policies to enhance population health.
Geriatric Exercise Science: Enhancing Health in Aging Populations
Geriatric exercise science focuses on promoting health and functional independence in older adults through exercise and physical activity. This research area explores topics such as the effects of exercise on age-related declines in muscle strength, balance, and mobility, the role of physical activity in preventing age-related chronic diseases, and the development of exercise programs for older adults with specific health conditions. Investigating geriatric exercise science can provide valuable insights into maintaining health and well-being in aging populations and improving the quality of life for older adults.
The field of physical fitness research offers a vast array of topics to explore, ranging from exercise physiology and psychology of physical activity to sports nutrition, injury prevention and rehabilitation, exercise prescription and programming, biomechanics and movement analysis, environmental and occupational health, public health and health promotion, and geriatric exercise science. By choosing a research topic that aligns with your interests and career aspirations, you can contribute to the advancement of knowledge in the field while gaining a deeper understanding of the intricacies of physical fitness. Embrace the opportunities that physical fitness research presents and let your passion for health science drive your exploration of these captivating topics.
Choosing Physical Fitness Research Paper Topics
Selecting an engaging and relevant research topic is a crucial step in the process of writing a research paper on physical fitness. With a wide range of possibilities within the field, it can be challenging to narrow down your focus and identify a topic that aligns with your interests and academic goals. In this section, we will provide expert advice on how to choose physical fitness research paper topics that are compelling, meaningful, and contribute to the existing knowledge in the field.
- Identify Your Interests : Start by reflecting on your personal interests within the realm of physical fitness. Consider the aspects of exercise, health, performance, or well-being that fascinate you the most. Are you passionate about exercise physiology, psychology of physical activity, sports nutrition, injury prevention and rehabilitation, exercise prescription and programming, biomechanics and movement analysis, environmental and occupational health, public health and health promotion, or geriatric exercise science? By identifying your interests, you can focus on areas that resonate with you and spark your curiosity.
- Stay Informed : Keep up-to-date with the latest research and advancements in the field of physical fitness. Subscribe to academic journals, attend conferences, and follow reputable websites and research institutes dedicated to exercise science. By staying informed, you will gain insights into current trends, emerging topics, and gaps in knowledge that may inspire your research interests.
- Conduct a Literature Review : Before finalizing your research topic, conduct a comprehensive literature review to explore existing studies, theories, and gaps in knowledge. Identify areas where further research is needed or where conflicting findings exist. A literature review will help you refine your research question and ensure that your topic contributes to the existing body of knowledge.
- Consult with Faculty or Experts : Reach out to your faculty members or experts in the field for guidance and advice. They can provide valuable insights, suggest potential research directions, and help you refine your research topic. Utilize their expertise to gain a deeper understanding of the field and identify relevant research questions.
- Consider Practical Applications : Think about the practical applications and implications of your research topic. How can your findings contribute to real-world situations, enhance practice, or inform policy decisions? Identifying the practical significance of your research can add value and relevance to your study.
- Balance Specificity and Feasibility : Strive for a research topic that is specific enough to provide depth and focus but also feasible within the constraints of your research project. Consider the available resources, time, and access to data or participants when determining the scope of your research topic. Finding the right balance will ensure that your research is manageable and achievable within the given timeframe.
- Collaborate and Network : Collaborate with peers, researchers, or professionals in the field to broaden your perspective and generate new ideas. Engaging in discussions and exchanging thoughts with others can spark creativity and open doors to potential research collaborations.
- Think Outside the Box : Don’t be afraid to think outside the box and explore innovative or unconventional research topics within physical fitness. Consider interdisciplinary approaches or emerging areas of research that intersect with exercise science, such as technology, digital health, or social determinants of health. Embracing innovative ideas can lead to exciting discoveries and contribute to the evolution of the field.
- Consider Ethical Considerations : When choosing a research topic, consider the ethical implications and potential risks associated with your study. Ensure that your research adheres to ethical guidelines and protects the rights and well-being of participants. Consulting with ethics committees or institutional review boards can help ensure that your research is conducted ethically and responsibly.
- Seek Feedback and Refine Your Topic : Once you have identified a potential research topic, seek feedback from mentors, peers, or academic advisors. They can provide constructive criticism, suggest modifications, or help you clarify your research objectives. Use their input to refine your research topic and ensure that it aligns with your academic goals and the requirements of your research paper.
Choosing a research topic in the field of physical fitness requires careful consideration and alignment with your interests, academic goals, and the existing knowledge in the field. By following these expert tips, you can select a compelling research topic that contributes to the advancement of knowledge, engages your passion, and offers opportunities for meaningful exploration. Embrace the journey of research and let your curiosity drive you to uncover new insights in the fascinating world of physical fitness.
How to Write a Physical Fitness Research Paper
Writing a research paper on physical fitness requires careful planning, organization, and adherence to academic conventions. In this section, we will provide you with expert advice on how to write a compelling and well-structured physical fitness research paper. By following these guidelines, you can effectively communicate your research findings, contribute to the existing body of knowledge, and showcase your understanding of the subject matter.
- Define Your Research Objective : Start by clearly defining the objective of your research paper. What is the specific question or problem that your study aims to address? Clearly articulate your research objective to guide your literature review, data collection, and analysis.
- Conduct a Comprehensive Literature Review : Before diving into the writing process, conduct a thorough literature review to familiarize yourself with existing research on the topic. Identify key theories, methodologies, and findings that will inform your study. Analyze and critically evaluate the literature to identify gaps in knowledge that your research can fill.
- Develop a Solid Research Methodology : Outline your research methodology, including the study design, sample size, data collection methods, and data analysis techniques. Clearly explain how you will collect and analyze data to answer your research question. Ensure that your methodology is rigorous, ethical, and aligned with the standards of your academic institution.
- Organize Your Paper : A well-organized research paper follows a logical structure. Start with an introduction that provides background information, states the research question, and outlines the significance of your study. Follow this with a literature review that synthesizes existing research and highlights the gaps in knowledge. Next, present your research methodology, including the sample characteristics, data collection procedures, and statistical analysis methods. Present your findings in a clear and concise manner, using tables, graphs, or charts as appropriate. Finally, conclude your paper by summarizing your findings, discussing their implications, and suggesting avenues for future research.
- Write Clearly and Concisely : Use clear and concise language to convey your ideas. Avoid jargon or technical terms that may be unfamiliar to your readers. Explain complex concepts in a way that is accessible to a broad audience. Ensure that your writing is well-structured, with paragraphs that flow logically and smoothly.
- Support Your Arguments with Evidence : Back up your arguments and claims with credible evidence. Use scholarly sources, peer-reviewed articles, and reputable databases to support your statements. Include proper citations and references to acknowledge the work of other researchers and avoid plagiarism.
- Analyze and Interpret Your Findings : Once you have collected and analyzed your data, interpret the results in the context of your research question. Discuss the implications of your findings and consider alternative explanations or limitations of your study. Engage in critical thinking and provide thoughtful insights based on your analysis.
- Address Limitations : Acknowledge the limitations of your study and discuss potential sources of bias or confounding factors. This demonstrates a critical understanding of the research process and adds credibility to your work. Suggest areas for future research that can overcome these limitations and contribute to further knowledge in the field.
- Follow Proper Formatting and Citation Style : Adhere to the formatting guidelines specified by your academic institution or the journal you intend to submit your research paper to. Use the appropriate citation style, such as APA, MLA, or Chicago, and ensure consistency throughout your paper. Pay attention to details, such as margins, font size, headings, and references.
- Revise and Edit : Before submitting your research paper, revise and edit it thoroughly. Check for grammar and spelling errors, sentence structure, and overall coherence. Read your paper aloud or ask a colleague to review it for clarity and flow. Make necessary revisions to improve the quality and readability of your paper.
Writing a physical fitness research paper requires careful planning, diligent research, and effective communication of your findings. By following these guidelines, you can craft a well-structured and informative paper that contributes to the field of physical fitness. Embrace the process of writing and view it as an opportunity to share your knowledge, insights, and passion for the subject matter. With dedication and attention to detail, your research paper can make a valuable contribution to the body of knowledge in physical fitness.
iResearchNet’s Writing Services
When it comes to writing a high-quality and impactful physical fitness research paper, having the right support and resources can make all the difference. iResearchNet is here to help you excel in your academic journey by offering a range of professional writing services tailored to your specific needs. Our team of expert writers, extensive research capabilities, and commitment to excellence ensure that you receive a top-notch custom paper that meets the highest academic standards. In this section, we will explore the key features and benefits of iResearchNet’s writing services, empowering you to make an informed decision and take your research paper to the next level.
- Expert Degree-Holding Writers : At iResearchNet, we understand the importance of expertise and knowledge in producing outstanding research papers. That’s why our team consists of highly qualified writers with advanced degrees in health science and related fields. They possess the necessary subject matter expertise to tackle even the most complex topics in physical fitness research. Our writers are experienced researchers themselves, allowing them to bring a unique perspective and in-depth understanding to your paper.
- Custom Written Works : Every research paper we deliver is customized to meet your specific requirements. We take into account your instructions, guidelines, and desired outcomes to create a paper that aligns with your academic goals. Our writers follow a systematic approach, conducting thorough research, analyzing data, and crafting a coherent and well-structured paper tailored to your research question.
- In-Depth Research : We believe that in-depth research is the cornerstone of a successful research paper. Our writers are skilled in conducting comprehensive literature reviews and accessing a wide range of scholarly sources. They stay up-to-date with the latest research findings, ensuring that your paper reflects the most current knowledge in the field of physical fitness. With access to reputable databases and libraries, our writers gather relevant and credible information to support your arguments and enhance the overall quality of your paper.
- Custom Formatting : Proper formatting is crucial in academic writing, and our writers are well-versed in various formatting styles, including APA, MLA, Chicago/Turabian, and Harvard. They meticulously adhere to the formatting guidelines specified by your academic institution, ensuring that your paper is professionally presented and meets the required citation standards.
- Top Quality : At iResearchNet, we prioritize delivering top-quality research papers that exceed your expectations. Our rigorous quality assurance process includes thorough proofreading, editing, and plagiarism checks to ensure that your paper is flawless and original. We are committed to maintaining the highest standards of quality and academic integrity in all our deliverables.
- Customized Solutions : We understand that each research paper is unique, and we tailor our services to meet your specific needs. Whether you require assistance with topic selection, literature review, data analysis, or complete paper writing, our team is flexible and adaptable to your requirements. We collaborate closely with you throughout the process, allowing for customization and ensuring that your paper reflects your research objectives and personal writing style.
- Flexible Pricing : We offer flexible pricing options to accommodate your budget and academic needs. Our pricing structure takes into account factors such as the complexity of the research paper, word count, and deadline. We strive to provide affordable services without compromising on quality, making our writing solutions accessible to students at various academic levels.
- Short Deadlines : We understand the pressures of tight deadlines, and our team is equipped to handle even the most urgent requests. With our short turnaround time of up to 3 hours, we can assist you in meeting those time-sensitive deadlines without compromising on the quality of your paper. Our writers are accustomed to working under tight schedules and are committed to delivering your research paper on time.
- Timely Delivery : Meeting deadlines is a top priority for us. We understand the importance of submitting your research paper on time, and our team is dedicated to ensuring timely delivery. Our efficient workflow, effective communication, and commitment to punctuality guarantee that you receive your paper within the agreed-upon timeframe.
- 24/7 Support : We provide round-the-clock support to address any questions or concerns you may have during the writing process. Our friendly and knowledgeable customer support team is available 24/7 to assist you with any queries, updates, or clarifications regarding your research paper. We value open and prompt communication to ensure a seamless experience for our clients.
- Absolute Privacy : Your privacy is of utmost importance to us. We take stringent measures to protect your personal information and ensure confidentiality. Our secure platform and strict privacy policy safeguard your data and ensure that your identity remains anonymous throughout the entire process.
- Easy Order Tracking : We provide a user-friendly order tracking system that allows you to monitor the progress of your research paper. You can easily check the status, communicate with your assigned writer, and receive regular updates on the development of your paper. Our transparent process keeps you informed and engaged throughout the writing journey.
- Money Back Guarantee : We are confident in the quality and reliability of our services. In the rare event that you are not satisfied with the final research paper, we offer a money-back guarantee. Your satisfaction is our priority, and we strive to address any concerns or issues to ensure your complete satisfaction.
iResearchNet is your trusted partner in writing exceptional research papers in the field of physical fitness. Our team of expert writers, commitment to quality, and dedication to your academic success set us apart. By choosing iResearchNet, you gain access to a range of professional writing services that are customized to your specific needs. Let us support you in crafting a high-quality, well-researched, and impactful research paper that showcases your knowledge and contributes to the field of health science. Place your order today and experience the difference iResearchNet can make in your academic journey.
Ready to Excel in Your Research Paper?
Are you feeling overwhelmed by the prospect of writing a research paper on physical fitness? Don’t worry, iResearchNet is here to help. Our team of expert writers, extensive research capabilities, and commitment to excellence make us the ideal partner for your academic success. Take advantage of our custom writing solutions and unlock your potential to deliver a top-notch research paper that impresses your professors and stands out among your peers.
Don’t wait any longer. Take advantage of iResearchNet’s custom writing services and let us help you excel in your research paper on physical fitness. Our team of expert writers, commitment to quality, and dedication to your success make us the ideal choice. Place your order today and unlock your full potential. Your research paper will be in capable hands, allowing you to focus on other important aspects of your academic journey. Contact iResearchNet now and experience the difference we can make.
ORDER HIGH QUALITY CUSTOM PAPER

- Services Paper editing services Paper proofreading Business papers Philosophy papers Write my paper Term papers for sale Term paper help Academic term papers Buy research papers College writing services Paper writing help Student papers Original term papers Research paper help Nursing papers for sale Psychology papers Economics papers Medical papers Blog

154 Exercise Physiology Research Topics: Essay Ideas

As a scientific study of life, physiology deals with the mechanism of living organisms. It primarily focuses on the physical functions of organ systems, cells, individual organs, and biomolecules. It is the study of how the body works. By integrating both physics and chemistry, it tries to understand the factors that connect the body systems leading to its performance. This academic field also requires research for students. However, getting exercise research topics to choose from could be difficult. This is because there is numerous research existing in the field. This article offers custom topics in exercise physiology for your paper or essay. Before you access these topics, want to know how to create the best paper? Find details below:
Process of Writing a Good Research
Writing a good research requires your focus. It also requires a familiarity with the field which could make your research easier and successful. Thus, to overcome every basic challenge you may face before or during research, you can consider this process:
Choosing a Topic If you’ve been given an assignment, this could be a challenging part for you. To do this, discover what’s interesting to you. What is interesting to you will be enjoyable, which makes selecting a topic from all available information easy. You can try to be creative with how you craft the topic. Preliminary Research At this stage, you need to research to see if there is enough information on the subject you want to discuss. Having enough information helps you set the context in which your research will be founded. You can try encyclopedias and many other internet sources. You can even consult lectures online, textbooks, journals, articles, and many other sources to readjust the focus of your topic. Gather Relevant Materials Gathering relevant material is as important as the previous step. This is because the materials have the information which is required for the work you want to do. You must therefore source your materials from online libraries and offline libraries. Because you’re writing on physiology, you may need to speak to trainers too, depending on what your topic is all about. Read and Take Notes Now, you can either engage in thorough reading during the research or breeze through the materials. However, it’s profitable if you check the table of contents to find the section of a book or journal which particularly discusses related topics of your research. When you do this, you get to read what is essential, ignoring others. While you read, you should also take notes. Taking notes lets you know the major points you want to build your arguments on. This could even help you with referencing and bibliography. Write This is where you organize your information and arguments. This doesn’t mean you should copy or plagiarize what you’ve read. It simply means writing what you understand after moments of creative assessment. Don’t try to get it right on the first attempt. There is room for drafts and revisions. Referencing Citing your sources properly shows that you didn’t plagiarize. An academic paper cannot be sourced from the author’s experience alone so you need to document where you got the information. To properly do this, know the required referencing format your institution or department prefers. There is MLA, APA style, Harvard, and many others. Understand the formats and reference your sources. This makes your professors and teachers believe you didn’t plagiarize another author. Proofread This is the final stage where you go through your paper again. You may do it once or five times. It depends on how satisfied you are with your paper. Proofreading is the stage where you assess your grammar or spelling errors as well as your punctuation weaknesses. It is also the stage where you ensure that the information you needed to share was passed across as you wanted it.
So, writing a paper for a high grade is not an easy task. It’s better to hire a professional writer and get your custom research paper complete on time.
How to Structure a Physiology Research Paper
Structuring your research paper is another essential thing to consider while writing. The following tips will help you know how to properly structure your paper:
The Title Page This is a significant section in the process of writing your paper. This shows the readers what your topic is all about and it makes your paper clearer. This is also where you also add your name. The Abstract An abstract is the summation of your research and the paper you’ve written. While it comes up before the introduction, it is often written after all the paper is written. Your abstract gives a brief overview of your paper, what you discussed, the resolutions, and the key points readers must not forget about the research. Your Introduction This is where you capture the hearts of your readers, professors, or teachers. This stage is where you give detailed information on the background of your research, the objectives you aim to achieve, and the materials and methods to be used to achieve the results. Main Body This is where you share the results of your findings. At this juncture, you’ll state your arguments and discuss everything you have discovered. If your work will be groundbreaking, this is the section to pay particular attention to. Conclusion This is where you give a summary of everything you’ve discussed. You can also share the key points with your readers here, to refresh their memory about the most important things in your research. You can also include a way forward or an action you expect your readers or experts to take. References This section is where you document every source which was instrumental in the course of writing the paper. This has already been discussed earlier.
If this process seems too long and tiring for you, you should remember about the opportunity to buy custom research paper from our expert team who will be happy to help you save time and nerves.
Exercise Physiology Topics
As a student of physiology, you may find it difficult to find the topic you can easily write on. You need to write a paper but you have limited access to a stream of exercise physiology topics of interest. You can consider the following:
- How does exercise physiology help in fighting against obesity?
- Role of aerobic exercise in losing belly fat
- The importance of physical exercise s for heart rehabilitation
- How to address knee injuries in athletes
- The right diet for athletes
- Is an athlete’s diet different from footballers’ diet?
- What are the distinctions between male and female athletes?
- Examine the body’s capacity to adapt to pain during rigorous physical activities
- Discuss the health benefits of whole-grain diets to athletes
- Analyze the benefits of whole-grain diets to people trying to lose weight
- Examine the dangers of sprains
- How outdoor activities help with depression
- How sports can help create social relationships
- How autism symptoms can be alleviated through physical exercises
- Analyze the effect of caffeine in Exercise
- Discuss the connection between physical exercise and aggressiveness
- How physical activities affect neurons
- Why do people believe Asians cannot lead Africans in sport?
- What are the physical limitations of Performance in some sports
- Examine the performance level of Usain Bolt since the start of his career
- Analyze the importance of physical activities for athletes
- Discuss the physical activities for swimmers
- How can people enhance their energy levels?
- How can obese people stay motivated while losing weight?
- Are there alternatives to physical exercises?
- Examine the negative effects of bodybuilding
- What are the dangers of physical exercises on human cells
- Express the ability of physical exercise in fighting disease
- How does arterial stiffness affect the ability to exercise
- Discuss what kinesiology entails.
Exercise Physiology Topics of Interest
You can also discuss exercise science research topics that are of interest to you. These are advanced and custom topics in exercise science for every academic level. Consider:
- Motor teaching in kinesiology
- An analysis of muscle anatomy
- An analysis of hip biomechanics
- An assessment of muscle synergies
- Motor learning in kinesiology and results
- Benefits of jogging
- Benefits of alcohol reduction
- How physical exercises wrestle flu
- The role of physical exercises in staying healthy
- Why does the heart pound during jogging?
- Non-communicable diseases and their link with physical activities
- Assess how effective walking uphill is to walking downhill
- Best diets for working out
- How physical activities Improve moods
- Role of physical activities in curing anxiety
- Design physical activities hide for autistic children
- Daily exercise: is it a necessity?
- How physical exercises affect mental health
- What are the signs of stress?
- How do physical exercises affect cardiovascular health?
Exercise Science Research Topics
As physiology deals with the science of human physical activities, you need topics on exercise physiology. You can choose from any of the below for your creative paper:
- Main principles of kinesiology
- How kinesiology helps in biomechanics
- Kinesiology sport apps
- Recent discoveries which have made physiology easier to understand
- How athletes can improve through kinesiology
- The role of kinesiology in orthopedic activities
- An in depth overview of how exercise by principle has worked so far
- How doctors achieve muscle movements for patients
- Suggested exercises for muscle development
- Suggested exercises for better body shape
- Why men are aggressive than women in bodybuilding
- The composition of the human bones
- Analyze the human skeleton
- Which muscle powers the leg of an athlete?
- How can performance be assessed on the track?
- Discuss how to increase flexibility
- Is dancing a sport?
- The biomechanics involved in running
- A guide to staying in the correct posture while working out
- The effects of incorrect postures while working out
- Why should exercises be consistent?
- What are the movements that activate the muscle?
- Suggestions to a long-distance athlete
- Suggestions to a short distance athlete.
Exercise Physiology Project Ideas
Do you want to write a project? There are numerous exercise physiology paper topics to base your project on. You can consider these:
- Five exercises to try with a team
- 5 exercises to try alone
- An analysis of any three exercises and what they do to the body
- How to improve health and physical fitness
- Sports supplements: discuss
- Is there a thing as over-working out?
- The benefits of physical fitness to pregnant women
- Physical fitness: effects on retired boxers
- Physical fitness: the cause of sagging bodies
- How to maintain physical shape in old age
- Why should anyone do physical exercise?
- Does physical exercise help with learning abilities?
- Why should shoes be worn during workouts?
- How to prevent sports injuries?
- How physical activities help college students’ academic prowess
- Role of physical exercise in boosting immune systems
- How can exercises prevent diabetes?
- How can exercises make bones recover early?
- The role of physiotherapy in sports
- Why do people need a fitness tracker?
- The role of tech in physiology
- Importance of vitamins in sports and exercises
- Why do you need to jot your fitness journey?
- Features of the best running shoes
- Does the sun help the body during workouts?
Exercise Physiology Research Paper Topics
Physiology and physical exercises are also connected to mental health strength. This is why you may want to consider these physiology research topics:
- Effects of video games
- Role of video games in physical activities motivation
- What can mitigate sport performance?
- Things to avoid while preparing for a football match
- Things to avoid why preparing for a race
- Why should athletes in preparation for a game avoid sex?
- Does alcohol affect an athlete’s performance 24 hours after drinking?
- The factors of the body responsible for Flexibility
- The consequence of a prolonged training period
- How sport-related injuries can affect interest in physical activities
- Examine how bones develop
- Discuss the physical exercise of humans and any animal of your choice and examine the distinctions
- The consequence of running barefoot
- How to properly plan your meal
- Healthy diets in UK schools
- Healthy diets in US schools
- Healthy diets in low-income countries’ schools
- How physical activities affect the nervous systems
- How physical activities impact the psychology
- How are skeletons kept balanced?
- Give an overview of the elderly persons’ health performance in Europe
- Protein a bodybuilder should consume?
- The predictable movement patterns causing Injuries
- How physical exercises help with muscle contraction
- How physical activities make people age.
Interesting Topics in Exercise Physiology
Would you like to consider something interesting for your paper or essay? You can dig through existing research related to some topics below and express yourself on exercise physiology. You can choose any of these great exercise physiology project ideas:
- The psychology in kinesiology
- Role of psychology in physical fitness
- How kinesiology helped in building prosthetics
- Exercise for injured war veterans
- How to keep fit after a long break
- How physical exercises can cause stress
- How physical exercise can strain
- The challenge facing men on getting abs
- How to build your abs
- An overview of controversial published physiology papers
- How to avoid belly fats
- Does the body go back to its earlier shape when you stop working out?
- How to empower your leg through exercises
- How to empower the arm through exercises
- How to train for biceps
- How to discover the best bodybuilders
- Are online bodybuilding activities functional as offline bodybuilding activities?
- An overview of recent discovery on exercise science
- What is most important to a basketballer?
- What training routine is most important to a boxer?
- What is the importance of warming up?
- How effective is bike riding?
- What does cross-fit training mean?
- How to retain training strength
- What are the training routines to stick to?
- Examine what plyometric exercises mean
- Spinning classes and their advantages
- Why people should work on their shoulders
- The importance of chest workouts
- Can yoga be called a type of physical exercise?
Need Research Paper Help?
Do you need writing services for your research papers? Our experts offer cheap prices for quality papers. If you’re amongst those who say “I want to pay someone to write my research paper “, you can hire us online. We are a writing company based online. With years of experience, we have been students’ most reliable and trustworthy writing service within and outside America. For your paper help, our writers are teachers, professors, and researchers with years of expertise in physiology research. They provide high quality work that could help you secure top marks and top your class in the process. Contact us with a “ do my research paper now” request and get an A+.
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
Terms & Conditions Loyalty Program Privacy Policy Money-Back Policy
Copyright © 2013-2024 MyPaperDone.com
221+ Interesting Kinesiology Research Topics (Updated 2024)

Move over to Motor Control, where researchers unravel how our brains orchestrate movement, influencing skills like playing instruments or even everyday tasks like typing. Or explore the depth of Sports Psychology, understanding the mind’s role in athletic performance, from motivation to mental toughness.
From Rehabilitation Kinesiology to Cardiopulmonary Kinesiology, investigating the heart and lungs’ function each category branches into fifteen unique research topics. Picture a wealth of discoveries waiting in each field, inviting everyone to explore the wonders of human movement in simple, captivating ways.
10 Step Guide For Selecting The Most Suitable Kinesiology Research Topics
Table of Contents
Going on a research journey in Kinesiology begins with the crucial step of choosing the right topic. With its diverse disciplines having human movement, exercise science, and health, selecting a compelling research topic is major Here are ten strategic steps to guide your search for a meaningful and impactful research topic in the field of Kinesiology and they are:
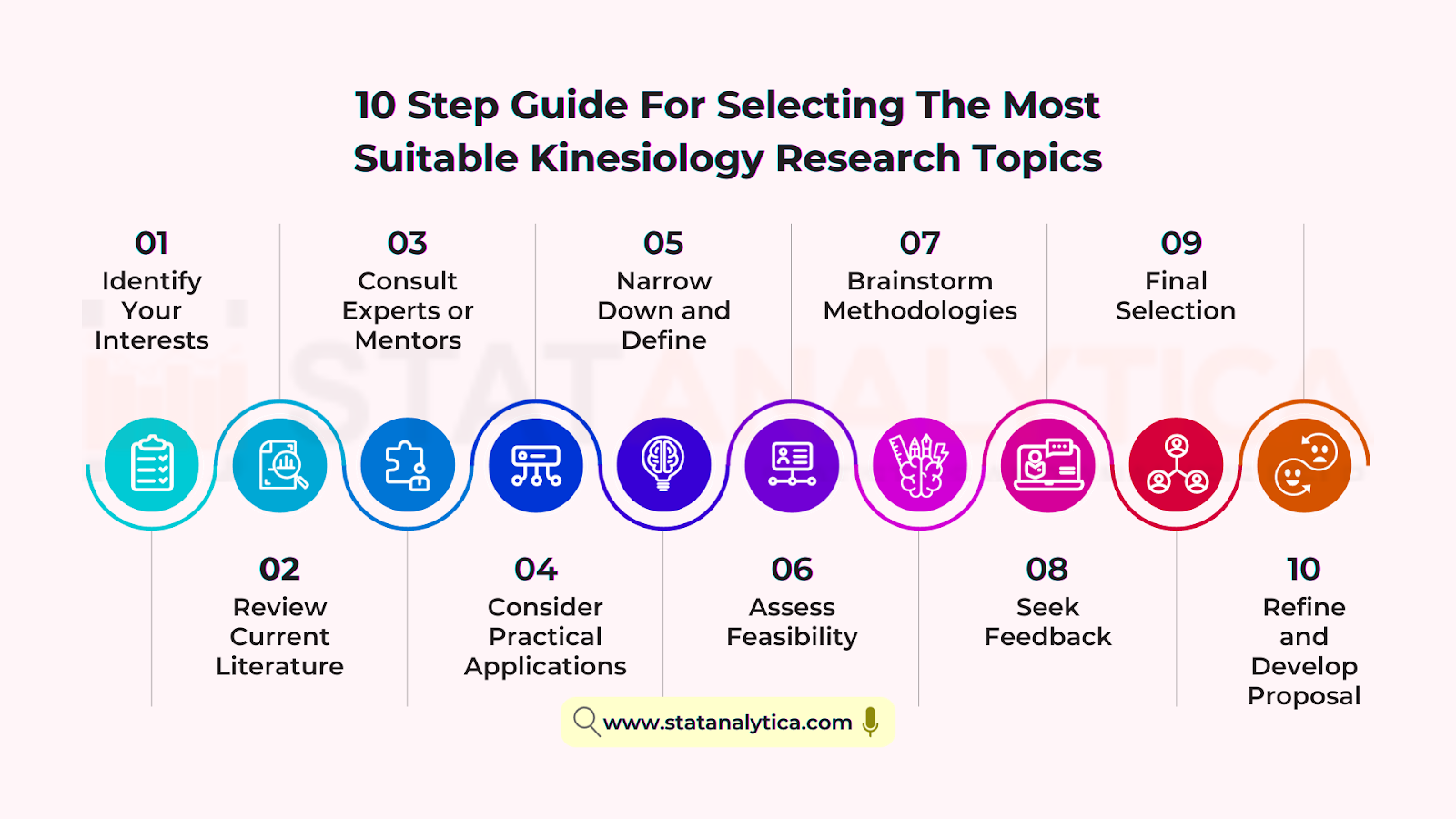
- Identify Your Interests
Start by exploring your own interests within Kinesiology. What aspects of human movement, exercise science, or physical activity intrigue you the most? Consider areas like biomechanics, exercise physiology, sports psychology, rehabilitation, or specific populations like pediatric or geriatric Kinesiology.
- Review Current Literature
Run a proper review of existing research in Kinesiology. Look for gaps, unanswered questions, or emerging trends in the field. Pay attention to recent publications and ongoing debates that could spark new research ideas.
- Consult Experts or Mentors
Engage with professors, experts, or mentors in Kinesiology. Discuss your interests and potential research areas with them. Their insights and experience can help refine your ideas and suggest valuable directions for exploration.
- Consider Practical Applications
Evaluate the practical applications of potential research topics. How might your research contribute to improving sports performance, enhancing rehabilitation methods, preventing injuries, or promoting health and wellness?
- Narrow Down and Define
Once you’ve gathered ideas, narrow down your options to a few specific research topics. Define these topics clearly, ensuring they are focused and researchable within a reasonable scope.
- Assess Feasibility
Consider the feasibility of each research topic. Evaluate factors such as access to resources, equipment, participants (if human subjects are involved), time constraints, and ethical considerations.
- Brainstorm Methodologies
Outline the methodologies you might employ for each potential research topic. Consider whether quantitative analysis, qualitative studies, experiments, surveys, or a combination would best suit your research objectives.
- Seek Feedback
Share your shortlisted research topics with peers or academic advisors for feedback. Their perspectives can help refine your ideas and identify any overlooked aspects.
- Final Selection
Based on the feedback received and your own evaluation, select the research topic that aligns best with your interests, feasibility, available resources, and potential impact in the field of Kinesiology.
- Refine and Develop Proposal
Once you’ve chosen a research topic, refine it further into a clear research proposal. Define your research questions, objectives, methodology, and expected outcomes in detail.
These steps can guide you through the process of selecting a research topic in Kinesiology, making sure that you select a topic that aligns with your interests and has the potential for meaningful contributions to the field.
Kinesiology Research Topics: 2024
Let us start this interesting journey and we will be guided by 15 categories and more than 221 kinesiology research topics. Here they are:
Top 15 Topics on Biomechanics
- Gait Analysis in Biomechanics
- Biomechanics of Human Movement
- Biomechanical Factors in Sports Performance
- Musculoskeletal Biomechanics
- Biomechanics of Injury Prevention
- Biomechanical Modeling and Simulation
- Biomechanics of Running and Sprinting
- Biomechanical Analysis of Lifting and Carrying
- Biomechanics of Balance and Stability
- Biomechanics of Joint Kinematics
- Biomechanical Assessment in Rehabilitation
- Biomechanics of Exercise Equipment Design
- Biomechanics of Occupational Movements
- Biomechanics of Biomedical Devices
- Computational Biomechanics
Top 15 Topics on Exercise Physiology
- High-Intensity Interval Training (HIIT) Effects
- Endurance Training and Adaptations
- Metabolic Responses to Exercise
- Exercise and Cardiovascular Health
- Effects of Resistance Training on Muscle Strength
- Exercise-Induced Fatigue Mechanisms
- Exercise and Hormonal Responses
- Environmental Influences on Exercise Performance
- Oxygen Uptake and Exercise Capacity
- Exercise and Immune Function
- Heat Stress and Exercise Performance
- Exercise and Aging: Sarcopenia
- Nutritional Strategies for Exercise Performance
- Exercise and Mental Health
- Gender Differences in Exercise Physiology
Top 15 Kinesiology Research Topics on Motor Control
- Neural Mechanisms of Motor Control
- Motor Learning in Skill Acquisition
- Motor Control and Aging
- Developmental Motor Control
- Brain-Computer Interfaces in Motor Control
- Neuroplasticity and Motor Control
- Motor Control in Rehabilitation
- Motor Control in Sports Performance
- Robotics and Motor Control
- Sensory-Motor Integration
- Motor Control in Parkinson’s Disease
- Spinal Cord Injury and Motor Control
- Computational Modeling of Motor Control
- Motor Control and Cognition
- Electrophysiology of Motor Control
Top 15 Topics on Sports Psychology
- Psychological Factors in Athletic Performance
- Team Dynamics in Sports
- Mental Skills Training for Athletes
- Psychological Strategies for Injury Rehabilitation
- Motivation and Sports Performance
- Coach-Athlete Relationship
- Stress and Coping in Sports
- Leadership in Sports Teams
- Burnout and Overtraining in Athletes
- Psychology of Peak Performance
- Goal Setting and Achievement in Sports
- Sportsmanship and Ethics in Athletics
- Psychological Resilience in Athletes
- Anxiety and Performance in Sports
- Psychological Interventions in Sports Coaching
Top 15 Topics on Rehabilitation Kinesiology
- Adaptive Technologies in Rehabilitation
- Neurorehabilitation Techniques
- Biomechanics of Rehabilitation
- Gait Analysis and Rehabilitation
- Assistive Devices in Rehabilitation
- Exercise Prescription in Rehabilitation
- Musculoskeletal Rehabilitation Strategies
- Rehabilitation in Sports Medicine
- Cognitive Rehabilitation in Kinesiology
- Virtual Reality in Rehabilitation
- Pediatric Rehabilitation Kinesiology
- Psychosocial Aspects of Rehabilitation
- Strength Training in Rehabilitation
- Balance and Coordination in Rehabilitation
- Occupational Rehabilitation Strategies
Top 15 Kinesiology Research Topics on Cardiopulmonary Kinesiology
- Exercise Physiology and Cardiopulmonary Function
- Cardiorespiratory Adaptations to Exercise
- Pulmonary Rehabilitation in Chronic Diseases
- Cardiopulmonary Exercise Testing
- Exercise Prescription for Cardiopulmonary Health
- Respiratory Muscle Training
- Cardiopulmonary Rehabilitation in COPD
- High-Altitude Adaptations in Cardiopulmonary System
- Exercise Interventions for Cardiovascular Health
- Respiratory Physiology during Exercise
- Cardiopulmonary Function in Athletes
- Pulmonary Gas Exchange during Exercise
- Cardiopulmonary Function in Aging
- Exercise-Induced Asthma and Cardiopulmonary Response
- Cardiopulmonary Rehabilitation in Heart Failure
Top 15 Topics on Biomedical Engineering in Kinesiology
- Wearable Technology for Movement Analysis
- Biomechanical Modeling in Prosthetics
- Biomaterials for Orthopedic Applications
- Biomechanical Assessment of Implants
- Biofeedback Systems in Rehabilitation
- Robotics in Assisted Movement
- Biomedical Sensors for Performance Monitoring
- Assistive Devices for Motor Impairments
- Biomechanics of Human-Machine Interfaces
- Biomedical Engineering in Sports Equipment
- Virtual Reality in Motor Rehabilitation
- Bio-inspired Design in Kinesiology
- Biomechanical Analysis in Ergonomics
- Computational Modeling for Injury Prevention
- Bioelectronic Systems for Movement Enhancement
Top 15 Topics on Aging and Kinesiology
- Effects of Exercise on Aging
- Aging and Musculoskeletal Health
- Mobility and Functional Decline in Aging
- Balance and Fall Prevention in Older Adults
- Exercise Interventions for Age-Related Diseases
- Cognitive Function and Aging
- Nutrition and Aging-Related Changes
- Strength Training in Older Populations
- Cardiovascular Health in Aging
- Longevity and Physical Activity
- Technology for Active Aging
- Social Factors and Physical Activity in Aging
- Bone Health and Aging
- Hormonal Changes and Exercise in Aging
- Psychological Well-being in Aging Populations
Top 15 Topics on Occupational Kinesiology
- Ergonomics in the Workplace
- Occupational Biomechanics
- Work-Related Musculoskeletal Disorders
- Physical Activity Promotion at Work
- Occupational Health and Safety
- Job Demands and Physical Performance
- Workplace Interventions for Health
- Worksite Wellness Programs
- Physical Fitness and Job Performance
- Occupational Stress and Physical Activity
- Aging Workforce and Physical Function
- Movement Analysis in Occupational Settings
- Occupational Therapy Interventions
- Workplace Design and Movement Optimization
Top 15 Kinesiology Research Topics on Neurological Kinesiology
- Stroke Rehabilitation in Neurological Kinesiology
- Neuroplasticity and Motor Recovery
- Spinal Cord Injury and Neurological Kinesiology
- Movement Disorders and Kinesiology
- Brain-Computer Interface in Neurological Kinesiology
- Parkinson’s Disease and Exercise Interventions
- Multiple Sclerosis and Kinesiology Interventions
- Neurological Kinesiology in Traumatic Brain Injury
- Neuromuscular Disorders and Kinesiology
- Cerebral Palsy and Motor Function in Kinesiology
- Vestibular Rehabilitation in Neurological Kinesiology
- Peripheral Nerve Injuries and Kinesiology Approaches
- Neurological Kinesiology and Gait Analysis
- Cognitive-Motor Interactions in Neurological Kinesiology
- Electromyography (EMG) in Neurological Kinesiology
Top 15 Topics on Paediatric Kinesiology
- Early Childhood Physical Development
- Motor Skill Development in Infants
- Pediatric Exercise Physiology
- Physical Activity and Cognitive Development
- Pediatric Obesity and Movement
- Motor Control in Children with Developmental Disorders
- Effects of Technology on Pediatric Movement
- Physical Activity Interventions in Schools
- Pediatric Sports Injuries and Prevention
- Motor Development in Preterm Infants
- Pediatric Rehabilitation and Movement Therapy
- Physical Literacy in Children
- Movement Assessment in Pediatrics
- Impact of Physical Activity on Academic Performance
- Neurological Development and Motor Skills
Top 15 Topics on Orthopaedic Kinesiology
- Biomechanics of Orthopaedic Injuries
- Orthopedic Surgical Interventions and Rehabilitation
- Muscle Function in Orthopedic Conditions
- Injury Prevention Strategies in Orthopedic Kinesiology
- Orthopedic Kinesiology in Athletes
- Gait Analysis in Orthopedic Patients
- Orthopedic Kinesiology and Joint Stability
- Orthopedic Kinesiology in Arthritis Management
- Orthopedic Kinesiology in Tendon and Ligament Health
- Neuromuscular Adaptations in Orthopedic Rehabilitation
- Orthopedic Kinesiology and Postural Stability
- Biomechanical Analysis of Orthopedic Devices
- Orthopedic Kinesiology and Cartilage Health
- Strength Training in Orthopedic Rehabilitation
- Orthopedic Kinesiology and Osteoporosis Management
Top 15 Kinesiology Research Topics on Ergonomics
- Workplace Ergonomics and Injury Prevention
- Human Factors in Ergonomics
- Ergonomics in Design and Engineering
- Ergonomic Assessment Methods
- Ergonomics in Healthcare Settings
- Ergonomics in Office Environments
- Ergonomics and Musculoskeletal Disorders
- Biomechanics and Ergonomics
- Ergonomics in Technology Use
- Ergonomic Interventions and Productivity
- Environmental Ergonomics
- Ergonomics in Transportation
- Ergonomics and Human-Computer Interaction
- Ergonomics in Manual Material Handling
- Anthropometry and Ergonomic Design
Top 15 Topics on Performance Enhancement
- Nutritional Strategies for Performance Enhancement
- Psychological Interventions in Performance Enhancement
- Strength and Conditioning Techniques
- Ergogenic Aids and Performance Enhancement
- Technology in Performance Enhancement
- Recovery Methods for Performance Enhancement
- Biomechanics for Performance Enhancement
- Endurance Training for Performance Enhancement
- Skill Acquisition for Performance Enhancement
- Environmental Factors in Performance Enhancement
- Periodization and Training Programs
- Genetics and Performance Enhancement
- Altitude Training and Performance Enhancement
- Hormonal Manipulation for Performance Enhancement
- Sleep and Performance Enhancement
Top 15 Kinesiology Research Topics On Physical Activity and Health
- Physical Activity and Cardiovascular Health
- Exercise and Metabolic Health
- Sedentary Behavior and Health Outcomes
- Physical Activity and Mental Health
- Exercise Interventions in Chronic Disease Management
- Physical Activity and Obesity
- Exercise and Bone Health
- Physical Activity and Cancer Prevention
- Exercise Prescription for Health Improvement
- Physical Activity and Immune Function
- Exercise and Stress Reduction
- Physical Activity and Cognitive Function
- Exercise and Aging-Related Health Issues
- Physical Activity and Diabetes Prevention Management
- Exercise and Respiratory Health
In conclusion, the diverse array of kinesiology research topics offers a wealth of fascinating areas to explore. From exercise physiology to sports psychology, and from biomechanics to motor learning, the field of kinesiology presents a rich variety of subjects to delve into. Whether investigating the impact of physical activity on mental health or exploring the intricacies of human movement, these topics provide ample opportunities for engaging discussions and valuable insights. By delving into these areas, individuals can gain a deeper understanding of the human body and its relationship to physical activity, paving the way for further discoveries and advancements in the field.
Related Posts

Step by Step Guide on The Best Way to Finance Car

The Best Way on How to Get Fund For Business to Grow it Efficiently
- Access Member Benefits

ACSM's Resource Library
From handouts to infographics, and tips to reduce high blood pressure to exercise recommendations for pregnant women, the Resource Library houses all free resources and is searchable by topic, format and audience. Access Resource Library
Access resources categorized by topic:
ACSM Fitness Trends Autism and Exercise Exercise Professional Resources Faculty/ Educator Resources Heart Health Mental Health Nutrition Physical Activity Guidelines Reducing Sedentary Behavior

ACSM's From Around the Field Webinar Series
ACSM’s From Around the Field science series gives students and professionals a chance to learn more about the diverse science ACSM members conduct. The informal discussions highlight what ACSM members study, the general research methodology they use and some of the interesting results their research generates.
Watch Presentations *Exclusive for ACSM members. Must be signed in with ACSM ID to access
- News Archive
- Certification Task Force
- Advertise with ACSM
- Current Partners
- Exercise is Medicine
- Rankings Archive
- Blogs and Resources
- National Youth Sports Health & Safety Institute
- Annual Report 2022
- Annual Report 2023
- Annual Report 2024
- Honor & Citation Awards
- Strategic Plan
- Student Membership
- Alliance Membership
- Professional-in-Training Membership
- Professional Membership
- Renew Membership
- Regional Chapters
- Member Code of Ethics
- ACSM Member Spotlight
- Group Exercise Instructor
- ACSM Personal Trainer Prep
- ACSM Exercise Physiologist Prep
- ACSM Clinical Exercise Physiologist Prep
- World Clinical Exercise Physiology Day
- Beijing Institute of Sports Medicine
- Wellness Academy
- Frequently Asked Questions
- Recertification FAQs
- Find an ACSM Certified Professional
- Certified Professional of the Year
- Wellcoaches
- Certified Professional Discounts
- Hire ACSM Certified Professionals
- Autism Exercise Specialist Course and Certificate
- Inclusive Fitness Specialist Certificate
- Online Education FAQs
- Approved Providers
- ACSM's Health & Fitness Journal
- Current Sports Medicine Reports
- Exercise and Sport Sciences Reviews
- Exercise, Sport, and Movement
- Medicine & Science in Sports & Exercise
- Translational Journal
- Paper of the Year Awards
- ACSM's Guidelines for Exercise Testing and Prescription
- ACSM's Resources for the Personal Trainer
- ACSM's Resources for the Exercise Physiologist
- ACSM's Clinical Exercise Physiology
- ACSM's Resources for the Group Exercise Instructor
- ACSM's Certification Review
- ACSM's Essentials of Exercise Oncology
- ACSM's Foundations of Strength Training and Conditioning
- ACSM's Nutrition for Exercise Science
- ACSM's Essentials of Youth Fitness
- ACSM's Introduction to Exercise Science
- ACSM's Health/Fitness Facility Standards and Guidelines
- ACSM’s Body Composition Assessment
- ACSM's Complete Guide to Fitness and Health
- Preparticipation Physical Evaluation (PPE) Monograph, 5th Edition
- ACSM's Fitness Assessment Manual
- ACSM's Exercise Testing and Prescription
- Textbook Adoption
- Translated Position Stands
- ACSM Official Statements
- Team Physician Consensus Statements
- Resource Library
- ACSM Fitness Trends
- Autism and Exercise
- Sudden Cardiac Arrest
- Mental Health
- Reducing Sedentary Behavior
- Sex Differences and Transgender Athlete Care
- Faculty Resources
- EIM Clinical Resources
- Black History Month
- ACSM's Brown Bag Series (archived)
- Physical Activity Guidelines
- Emerging Physician Leaders Pilot Program
- Annual Meeting
- IDEA & ACSM Health & Fitness Summit
- Advanced Team Physician Course
- Sports Medicine Essentials
- Integrative Physiology of Exercise Conference
- International Team Physician Course
- Regional Chapter Meetings
- Meeting Exhibits and Sponsors
- Research & Program Grants
- Howard G. "Skip" Knuttgen Scholar Award
- Travel and Research Awards
- ACSM Research Grant Recipients
- ACSM Travel Award Recipients
- Dedicated Endowments & Funds
- Planned Giving / Discovery Society

Home > Integrated Health Sciences > SCHOLARSHIP_KIN
Topics in Exercise Science and Kinesiology is dedicated to relaying information to the research practitioner in an open access format.
The journal publishes original research in two main practical areas: 1) the "Process of Science" (aspects surrounding scientific discovery and practice, which could include findings from investigations, novel scientific applications, or experience gained through completing research), and 2) "Implementation Strategies" (processes by which aspects can be applied to the performance or practice of exercise, including pre-exercise routines, novel training applications, or methods for improving performance). The journal accepts original research submissions in the following categories 1) Expedited Articles, 2) Review Articles, and 3) Case Studies.
The journal also publishes “Topics Briefs” which distills evidence-based information into a content format more easily implemented than the typical publication written for an academic audience. The aim of the TESK offering is to provide clear, digestible, and practical information for specific populations in the area of exercise science and kinesiology. If you have questions about where your work fits, please contact the editors .
See the Aims and Scope for a complete coverage of the journal.
To maintain a happy editorial board and reviewer pool, Topics in Exercise Science and Kinesiology will reduce our normal staffing during June and July. Any manuscripts submitted during these months may not begin the pre-review process until August. Additionally, manuscripts under review during these months may take longer than our normal time course to complete. It is suggested to submit well in advance of these months in order to avoid any delays.
Join the International Community of Scholars in Kinesiology for benefits on this and other journals.
Branded apparel and accessories are available for purchase here .
Current Issue: Volume 5, Issue 1 (2024)
Original research.
Acute Ingestion of Dark Chocolate Fails to Affect Running Economy in Recreational Female Runners Bianca J. De Lucia, Beau Kjerulf Greer, and Christopher B. Taber
Determining the barriers to the use of post-match fatigue monitoring in the rugby codes: A Concept Mapping study. Mitch Naughton, Tannath Scott, Dan Weaving, Scott McLean, and Colin Solomon
Establishing the Validity and Reliability of the Astroskin® Biometric Shirt Alex MacQuarrie, Jasmin Sidhu, Chloe Deetlefs, Steve Whitfield, and Matt Stainer
The Cardiorespiratory Response while Nordic Walking vs. Regular Walking Among Middle-Aged to Older Adults Thomas R. Atwood, Alyssa R. Horton, Natalie G. Hanson, Katelyn N. Moyer, Saori I. Braun, Nicholas M. Beltz, and Jeffrey M. Janot
Simultaneous Acute Stretching with Whole Body Vibration does not have an Additive Effect on Extensibility of the Hip Adductor Muscles Roger L. Hammer Dr., Peter V. Loubert, and Naveen Sharma
Incidence of Achilles Tendon Ruptures and Associated Factors in Women's Artistic Gymnastics Kayla Horton and Amanda Hawkes
Implementation Strategies
Breakaway Roping – Event Analysis and Resistance Training Model Andrew A. Wolfe, Libby E. Winchell, Ruth Caddell, Jackson Maynard, and Gillian Braden
Expedited Articles
Kinematic characteristics of novices’ sprint techniques at maximum velocity phase Saburo Nishimura and Yoshinori Kinomura
A Pilot Study on the Measurement of Connectedness to Nature Around Nature Immersion with Green Exercise on Desert Trails Dustin W. Davis, Elias M. Malek, Robert Salatto, Marcus M. Lawrence, Jacob W. Manning, Mark DeBeliso, Merrill Russen Landers, Graham McGinnis, and James W. Navalta
Review Article
Exploring the Mechanistic Trail Connecting Cellular Function, Health, and Athletic Performance With Phase Angle: A Review on the Physiology of Phase Angle and Exercise-Based Interventions Trevor Short and Paulette Yamada
- Journal Home
- About This Journal
- Aims & Scope
- Editorial Board
- Reviewer Rubric
- Submit Article
- Most Popular Papers
- Receive Email Notices or RSS
Advanced Search
ISSN: 2766-2187
Home | About | FAQ | My Account | Accessibility Statement
Privacy Copyright
7 Kinesiology Research Topics for a Dissertation
Kinesiology, the scientific study of human movement and physical performance, offers a broad array of research topics for dissertations. The field is evolving rapidly, with new findings and developments in exercise science, making it a rich ground for scholarly exploration. In this article, we’ll explore seven emerging kinesiology research topics, discuss how to formulate a dissertation topic, and outline what makes for a successful dissertation or research paper.
Research Topics for Kinesiology PhD Students
In a PhD program, students are expected to craft a unique dissertation that contributes to the field’s body of knowledge. Below are some detailed research topics for kinesiology PhD students, starting with biomechanics of injury prevention in sports.
1. Biomechanics of Injury Prevention in Sports
Injury prevention is a critical area in kinesiology. With the rise of high-intensity sports and physical exercise training programs, understanding the biomechanics behind injuries is crucial. Research can focus on identifying risk factors, developing new techniques or equipment to reduce injuries, or analyzing movement patterns that predispose athletes to specific injuries.
Formulation Tip: Narrow your focus to a particular sport or type of injury. For instance, “Biomechanical Analysis of ACL Injury Prevention in Female Soccer Players.”
2. Neuromuscular Adaptations to Strength Training
Neuromuscular adaptations are essential for improving athletic performance. This topic investigates how muscles and nerves adapt to different training regimens. Research can explore the differences in adaptations based on age, gender, or the type of strength and resistance training performed.
Formulation Tip: Consider a specific population or training method. For example, “Neuromuscular Adaptations in Elderly Adults Engaged in High-Intensity Interval Training.”
3. The Impact of Wearable Technology on Physical Activity and Health
Wearable technology, such as fitness trackers and smartwatches, has become ubiquitous in sport science. Research in this area can assess the accuracy of these devices, their impact on physical activity levels, and their potential to improve health outcomes.
Formulation Tip: Focus on a particular demographic or health outcome. For instance, “The Effectiveness of Wearable Fitness Trackers in Promoting Physical Activity Among Sedentary Office Workers.”
4. Psychological Factors in Athletic Performance
Exercise psychology plays a significant role in athletic performance. This research topic can delve into how mental health factors such as motivation, stress, and anxiety influence performance. It can also explore psychological interventions to enhance performance.
Formulation Tip: Choose a specific psychological factor and sport. For example, “The Role of Mental Toughness in Endurance Sports Performance.”
5. Exercise Physiology and Chronic Disease Management
Exercise physiology’s role in managing chronic diseases such as diabetes, cardiovascular disease, and obesity is a growing research area. Studies can take an in-depth look at how different types of exercise affect disease progression and management.
Formulation Tip: Target a specific chronic disease and exercise type. For instance, “The Impact of Aerobic Exercise on Blood Glucose Control in Type 2 Diabetes Patients.”
6. Gender Differences in Sports Performance
Gender differences in sports performance remain a contentious and highly researched topic. This area can explore physiological, biomechanical, and psychological differences between male and female athletes and how these differences influence training and performance.
Formulation Tip: Focus on a specific aspect of performance. For example, “Gender Differences in Recovery Rates Following High-Intensity Interval Training.”
7. The Role of Nutrition in Athletic Performance
Nutrition is fundamental to athletic performance. Research can investigate the effects and health benefits of various diets, sports supplements, and hydration strategies on performance and recovery. This area is particularly relevant given the proliferation of new dietary trends and supplements.
Formulation Tip: Focus on a specific nutrient or dietary approach. For instance, “The Effects of Ketogenic Diet on Endurance Performance in Long-Distance Runners.”
Formulating Your Dissertation Topic
When formulating your dissertation topic, consider the following steps during the research process:
- Identify Your Research Interests: Choose a topic that genuinely interests you, as you will be dedicating a significant amount of time and effort to this research.
- Conduct an Existing Literature Review: This helps you understand the current state of research and identify gaps that your dissertation can fill.
- Define Your Research Question: Your research question should be specific, measurable, achievable, relevant, and time-bound (SMART).
- Consult with Advisors: Seek input from your academic advisors and mentors to refine your potential kinesiology research paper topics to ensure their feasibility.
- Consider the Scope: Ensure that your topic is neither too broad nor too narrow. It should be manageable within the time frame and resources available.
What Makes for a Successful Dissertation?
A successful dissertation in kinesiology should possess the following qualities:
- Originality: Your research should contribute new knowledge or insights to the field.
- Relevance: The topic should address a significant issue or gap in current research.
- Methodological Rigor: Use appropriate and robust research methods to ensure the validity and reliability of your findings.
- Clarity: Your writing should be clear, concise, and well-organized. Each section should logically flow into the next.
- Comprehensive Literature Review: Demonstrate a thorough understanding of the existing research and how your work fits into the broader context.
- Strong Data Analysis: Employ rigorous data analysis techniques and clearly present your findings.
- Implications and Recommendations: Discuss the implications of your findings for practice, policy, and future research. Provide practical recommendations based on your results.
Contribute to the Field with CSP Global’s Kinesiology Program
Choosing a dissertation topic in kinesiology can be challenging but immensely rewarding. By focusing on emerging and relevant research areas, you can contribute valuable insights to the field. Whether it’s the biomechanics of injury prevention or the psychological factors influencing athletic performance, your research can have a significant impact. Remember to formulate your topic carefully, ensure methodological rigor, and contribute original knowledge to make your dissertation a success.
CSP Global offers 100% online doctoral programs in kinesiology. Earn your PhD or EdD in our student-centered online programs. CSP Global’s kinesiology doctoral programs are taught by world-class instructors and provide students with opportunities to gain real-world experience in the field of health sciences. Students can expect to learn deep research methods, complete a research dissertation, and graduate ready to advance their careers in kinesiology.
Level up by earning your doctorate from CSP Global. If you’re interested in learning more about earning a Doctorate in Kinesiology please contact us .
Request Information
An official website of the United States government
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Publications
- Account settings
- Advanced Search
- Journal List
Research In the Exercise Sciences; Where We Are and Where Do We Go From Here: Part II?
Kenneth m baldwin, fadia haddad.
- Author information
- Copyright and License information
Corresponding Author : Kenneth M. Baldwin, Ph.D., FACSM, Department of Physiology and Biophysics, University of California, Irvine, Irvine, CA 92697, Phone: 949-824-7192, Fax: 949-824-8540, [email protected]
This decadal perspective summarizes novel, insightful observations achieved in exercise science. The topics span genomics and gene function, epigenetics, cell signaling, epidemiological phenomena and other important areas. A future strategy is presented along two parallel, integrated paths involving: 1) a continuance of genomic discovery and gene function; 2) classical biochemical/ physiological approaches toward solving biological- and health/disease-related phenomena.
Keywords: gene regulation, muscle as an endocrine organ, epigenetics, cell signaling, biochemistry, epidemiology, obesity
Introduction
In 2000, a perspective was provided concerning of the evolution of the “exercise sciences” in the 21 st century ( 4 ). The article covered a wide range of topics such as: 1) emerging technologies and research initiatives; 2) new fields of research; 3) future funding trends and research priorities; 4) future challenges in exercise research-the building of a solid foundation; and 5) where the exercise sciences fit in health care.
Well, here we are 10 years later, and the current authors have been charged with the assignment of taking the pulse concerning the scope of progress that has been made in the exercise field in the last ten years along with projecting what impact such accomplishments bode for the future. Although the goal of this perspective will be essentially the same as before, we will take a slightly different tactic in formulating such a view. Rather than providing only our personal opinion, several experts in the field were contacted to provide their own insights. The responses received were quite insightful and there was a large degree of agreement in their respective viewpoints.
In the present article, the goal is to examine to what degree progress has been made on several fronts in the exercise field. Based on the dialogue presented below, it is not surprising that considerable advancements have occurred in skeletal muscle given the fact that it is the organ system of exercise/movement. Then, we will posture how the exercise field should evolve. Hopefully, such an approach will provide a reflection of what the science community has accomplished and how we can extend the knowledge base down the road. Furthermore, we apologize in advance for not providing more depth and breadth in covering topics beyond those highlighted in this perspective (see next section).
Selected Highlights and Novel Discoveries in the Last 10 Years
Before going into the details, it is important to point out some general background information. A Pub Med search with the word “exercise” retrieved ~82,826 peer reviewed articles published in the past 10 years. There were ~3836 papers linked to genetics; 45 to proteomics; 155 to genomics; 22 to epigenetics; 326 to signaling pathways. For additional links to the exercise theme: the term obesity retrieved 7357 articles; diabetes 6312; longevity 254; muscle 18,562; bone 4038; metabolism 24,033; nervous system 4505; hormones 6954; brain function 2644; circulation 3426; immune system 1281; respiratory 5734; and hematology 126. These data suggest a wide range of subject matter linked to the exercise sciences, and illustrate a vast group of investigators focusing on these important topics. Unfortunately, and as noted above, the authors cannot cover all these mentioned themes given the strict space constraints for this brief perspective.
Achievements in Gene Function and Regulation
Genomics, genetic factors and exercise.
The Human Genome Project was completed in 2003. No doubt, this milestone helped pave the way for genomic research exploring how genetic factors impact the responses and adaptations of health-related traits to exercise stimuli. Furthermore, studies have identified polymorphism in more than 239 genes and quantitative trait loci (QTL) and associated certain genotypes with cardiovascular responses, fitness phenotypes, as well as muscle strength and power adaptations ( 8 ). For example, there is a strong association between R577X genotype of the alpha actinin 3 gene (ACTN3) and performance in a variety of athletic endeavours. The R allele has been found to be associated with power-oriented performance, whereas the XX genotype may be linked with endurance ability ( 49 ). However, the collective data point to the fact that although some genotypes may be associated with certain phenotypes, the overall physiological significance is multifactorial and the result of interactions between the genome, the epigenome, and the environment, widely vary on an individual basis. Thus, this evolving field has generated a wide diversity of viewpoints as to how the field will evolve as pointed out by the excellent perspective provided by Stephen Roth, Ph.D., FACSM ( 42 ). He predicts that genomic studies will continue to enhance our understanding of the underlying biology of exercise responses. Genomic information can be useful for prescribing individualized exercise regimen especially when treating susceptible patients. No doubt, exercise genomics, applied in public health care, will be a hot area in the next decade.
Gene Knockouts
In the last 10 years the molecular manipulation of gene function, designed almost exclusively for the mouse, has exploded with a large number of the papers recently published in the last two years. The primary approached has been to null out a target gene and address the likely physiological and biochemical outcomes (phenotype) in the context of either acute or chronic exercise performance. The genes that have been studied span a broad scope, as illustrated by the following genes examined: triacylglycerol lipase, Insulin Like Growth Factor-1 (IGF-1), peroxisome proliferator-activated receptor gamma coactivator-1-alpha (PGC1-alpha), Adenosine Monophosphate (AMP) related kinases, desmin, Vascular Endothelial Growth Factor (VEGF), Tumor protein P53, carnitine functional interruption, Muscular Dystrophy (MDX), alpha1 AMP kinase, Uncoupling Protein-3 (UCP3), LOV keltch protein (LKP) kinase, thrombospondin-1 (TSP-1), myoglobin, myostatin, adenine nucleotide translocator, hypoxia inducible factor-1alpha to name a few.
To illustrate the power of this research approach the function of TSP-1 will be illustrated as reported by Malek and Olfert ( 28 ). This gene is a negative modulator of angiogenesis in several tissue types. Animals with this gene knocked out have greater muscle capillarity and a corresponding greater running endurance capacity than the wild type animals. This study thus provides a unique insight that the capillary-to-muscle interface is a critical factor that limits exercise capacity. Importantly, this paper points out that the negative consequences of the loss of TSP-1 must also be considered, as there are checks and balances to maintain optimal levels of physiological processes whether it is blood supply regulation or cell growth. In the context of the recent review article by Booth and Laye ( 7 ), this study would have been more complete if the animals were also studied under increased daily physical activity. Gene function may differ between inactive animals and those with high levels of daily physical activity ( 7 ). For example, with certain gene knockouts, animals fail to show the disease phenotype when the animals have access to voluntary wheel running ( 7 ). Thus for a full spectrum of gene function, knockout animals should be compared to wild type not only at rest but also under chronic exposure to physical activity and in response to an acute exercise stress stimulus ( 7 ).
RNA Interference (RNAi)
RNA interference (RNAi) is the process of sequence-specific post-transcriptional gene silencing, initiated by double-stranded RNA that is identical in sequence to the target gene. The discovery that synthetic duplexes of 21 nucleotides (siRNAs) trigger gene-specific silencing in mammalian cells has made them a useful tool to study gene function in mammalian systems ( 16 , 26 ). SiRNA technology involves the use of small interfering RNA fragments that can be delivered into cells either directly or via a plasmid vector delivery system. Once within the cell, siRNAs trigger the degradation of their cognate mRNA thereby reducing the substrate for translation. Thus, the target gene becomes significantly “knocked down” thereby reducing the effectiveness of the target gene’s regulation of physiological processes. This technology is theoretically simpler and more cost effective than genetically producing the ”knockout” approach and is particularly useful in studying function of genes that are lethal upon complete knockout. Another advantage of siRNA usage is that since the target protein is not completely eliminated, the knockdown perturbations are less likely to induce compensatory plasticity processes observed with complete knockouts. Consequently, in the future siRNA is predicted to be used in a broad range of experiments targeting the rat, because of its long standing use as an important animal model in the exercise field.
Epigenetics and Gene Regulation
Epigenetics is a new and rapidly growing research field that investigates heritable alterations in chromosome function/gene expression caused by mechanisms other than changes in DNA sequence. Epigenetic mechanisms are diverse but can be classified into three interacting areas involving: modulation of the chromatin/histone structure (methylation, acetylation, phosphorylation); DNA methylation; and noncoding RNA such as microRNA and antisense RNA; reviewed in ( 30 ). Recent studies have shown that epigenetic modulations can also be dynamically and rapidly occurring in response to environmental changes to alter gene expression. For example, our group, in carrying out recent studies on the plasticity of the myosin heavy chain (MHC) gene family in response to altered loading state, has discovered two types of epigenetic phenomena. The first involves the expression of antisense RNA in the fast MHC gene locus in which the MHC genes are organized in tandem on the same chromosome. These antisense RNAs allow adjacent genes to cross talk as well as to coordinate regulation of neighboring MHC genes ( 35 , 41 ). Second, we have discovered that repression of slow MHC and activation of fast MHCs (and vice versa) in a given muscle involve altered patterns of acetylation and methylation of the histones that regulate expression of MHCs, e.g. , slow to fast and fast to slow depending on the loading conditions ( 36 ).
Recently, epigenetic regulation was linked to rat behavior in response to exercise. It was shown that exercise causes epigenetic changes that lead to enhanced memory formation and better coping in response to stress. Significant increases in histone H3 phosphoacetylation and induction of the cFos gene were found in the brain of exercised rats ( 11 ). Another epigenetic inducer is diet. For example, recently, a high fat diet was shown to increase methylation of the leptin gene, thus reducing its expression in obese people ( 31 ). These findings raise the possibility that many of the adaptations that occur in muscle and in other organ systems in response to diet, exercise, chronic inactivity, aging, and many disease interventions could be regulated, in part, via epigenetic phenomena. These observations lead to an important topic for future investigation, which suggests the possibility that the beneficial effects of exercise is occurring via epigenetic reprogramming of gene expression. The notion that environmentally induced epigenetic traits have an impact on future generations has important ramifications for future research involving diet and exercise. For example, can diet and exercise induce specific epigenetic modulations which serve as countermeasure for many disorders, which helps in overcoming our genetic weakness and predisposition to certain diseases ( 7 )?
Micro-RNAs (miRNA) are small non-coding RNAs that regulate gene expression at the posttranscriptional level ( 44 ). These highly conserved, ~21-mer RNAs regulate the expression of genes by binding to the 3'-untranslated regions (3'-UTR) of specific mRNA. Each individual miRNA could act posttranscriptionally to target hundreds of mRNAs for translational repression, degradation or destabilization. They are involved in many aspects of cell function and play a significant role in disease development. Research suggests that miRNAs play major regulators of gene expression, and thus are part of the adaptive response ( 10 ). Computational analyses continue to identify gene targets for cellular miRNA; however, these targets must be validated with microarray data. MiRNAs together with transcription factors generate a complex combinatorial code regulating gene expression. There is speculation that in higher eukaryotes, the role of miRNAs in regulating gene expression could be as important as that of transcription factors. Thus, identifying and targeting miRNA-transcription factor gene networks may provide a potent approach in future research in Exercise Science as applied to therapy and disease prevention.
Genetic Selection and Maximal Exercise Performance
The relative contribution of genetic and environmental influences in terms of individual exercise capacity is difficult to determine in humans. In recent studies using self selected rodents after many generations (7 versus 15) it was possible to delineate key factors for determining maximal oxygen consumption rate (MOCR) in inherent high capacity runners (HCR) versus low capacity runners (LCR) independent of training stimuli. In generation 7 animals, MOCR was primarily differentiated between the two groups by the ability of the muscle system to extract and diffuse oxygen rather than the capacity to deliver oxygen. In generation 15 the opposite was apparent in that the HCR again had greater MOCR than LCR, but the difference in this generation was due to greater oxygen delivery rather than greater oxygen extraction. In both generations, HCR group had greater oxygen diffusion capacity. According to P. D. Wagner and associates ( 21 ), these unique studies are important in that they now allow researchers to dissect each step in the transport chain while also, eliminating the environmental factors contribution to these physiological phenomena.
Cell Signaling: and Regulatory Molecules Impacting Metabolism and Muscle Mass
Muscle metabolism.
One of the long standing questions in all fields of biomedical science involves filling in the gap between the stimulus and response to a given perturbation, e.g. , exercise (aerobic and/or resistance loading). In the last decade major strides have occurred in filling in such gaps and this is illustrated by a couple of examples, even though there are numerous signaling pathways that control physiological and immune homeostasis. In the metabolic fields relative to exercise, the signaling pathway centered on adenosine monophosphosphate kinase (AMPK) has shown that by activation of this so called “fuel gauge” or “metabolic regulator” (pharmacological and contraction induced activation), a number of outcomes occur in association with AMPK activation ( 47 ). These include increases in glucose disposal; fatty acid oxidation; activating transcriptional regulators of mitochondrial biogenesis; mediating actions of hormones such as leptin, adiponectin, and glucocorticoids. Interestingly, AMPK also serves as a negative modulator of anabolic processes (glycogen, fatty acid, and protein synthesis). Thus, AMPK is a powerful regulatory molecule and in the future it will likely be the target of various pharmacological interventions for treating various disorders centered on diabetes and obesity. In this context, we have witnessed the controversy of using pharmacological manipulation of AMPK function and its downstream targets (PPAR-delta and PGC1-alpha) as presented in the findings of Evans and associates on the improvement of exercise performance via an exercise “pill” ( 34 ). This paper has created several counter viewpoints as to the physiological impact and merit of such an approach as reviewed in the excellent article by Booth and Laye ( 7 ).
Mitochondrial Biogenesis
Forty two years ago John Holloszy, M.D., made a seminal discovery that programmed running exercise carried out over several weeks induces a doubling of the mitochondria in the leg muscles of rodents not normally accustomed to physical activity ( 18 ). Since that time hundreds of studies have focused on this important phenomenon, which serves as one of the key lynchpins that define the field of muscle plasticity. Fast forward to this decade, several studies as reviewed by Holloszy and Hood, respectively ( 19 , 20 ), provide the mechanism(s) driving this important discovery. For example, studies have shown that a single bout of exercise induces a rapid increase in mitochondrial biogenesis that is mediated by PGC1-alpha and other factors, which induce transcription of both nuclear and mitochondrial genes that combine to encode the protein comprising the mitochondria ( 3 , 25 ). This important discovery has rejuvenated the science community such that mitochondrial research in health, disease, and aging will be a major focus in the next decade. In fact a new field of science referred to as “mitochondrial medicine” has emerged.
Muscle mass
Another important discovery/advancement of similar importance involves the IGF-1- protein kinase B/AKT-mTOR (mammalian target of rapamycin) signaling pathway, which has been linked to anabolic processes, particularly in skeletal muscle in response to exercise ( 6 ). This pathway has been shown to activate a number of down stream effectors that act on enhancing expression of the ribosomal translation machinery, as well as increasing activity of activators and enzyme systems in the processes governing protein translation as well as immune function. Further, this system is linked to inhibiting processes Forkhead box 01 (Foxo1-Atrogin-1 MAFbx system) governing the catabolic processes of protein degradation ( 29 , 32 , 43 ). There are several other signaling pathways that have been dissected and worthy of being mentioned, but lack of space prevents such a dialogue in this brief review.
In the context of the above topics concerning signaling for metabolic regulation and the regulation of anabolic pathways for controlling muscle mass, a perspective has evolved suggesting that if the signaling pathway for metabolic control is activated, the pathway(s) for anabolic outcomes is down regulated and vice versa ( 2 , 12 ). This incompatibility seems counter intuitive to some degree since many athletes train for enhanced functional capacity for both properties. Clearly research in the future is needed to address this important topic.
Muscle as an Endocrine Organ System
In recent years Pedersen and associates ( 37 ) coined the term “myokine” for any factor apparently expressed/synthesized in skeletal muscle in response to physical activity, which in turn can act either locally or released into the blood to regulate function in other tissues. Three myokines have been identified and partially characterized. Interleukin-6 (IL-6) appears to act both locally on carbohydrate metabolism and distally on hormone activity in the pancreas/liver and in lypolysis in adipose tissue. IL-8, acts locally and may play a key role on angiogenic processes. IL-15, which is released during resistance exercise ( 40 ), appears to regulate anabolic processes in skeletal muscle. Interestingly, individuals expressing certain single nucleotide polymorphism in the IL-15 receptor-alpha, demonstrated more muscle hypertrophy than other subjects in response to resistance exercise training ( 40 ). These collective observations illustrate that this emerging field is ready to explode and will have a major impact on how we view the role of skeletal muscle in terms of being a regulator of function in other organ systems (see Fig. 1 ).

depicts two parallel tracts of research focus in exercise science: 1) genomics and gene regulation, and 2) basic biochemistry and physiology. These priorities should move synergistically with one another to insure that integrated function across several organ systems will unfold to derive the important outcomes of fitness, reduced disease potential, and longevity. The rationale for this scheme is depicted in the text material.
The Dynamics of Connective Tissue and Bone Adaptation With Exercise
The study of connective tissue-both in regards to tendon and the intramuscular connective tissue, recently has blossomed to the forefront due, in part, to the efforts of Kjaer’s group ( 27 ). It has been demonstrated that the metabolism, blood flow, and turnover of collagen in connective tissue is rapid and that regulatory factors are up regulated in relation to exercise (IGF-1, Transforming Growth Factor (TGF-beta, Il-6). By use of microdialysis and stable isotopes, ultrasonography, atomic force microscopy, these various approaches have made it possible to determine the structure and function of this dynamic tissue along with examining the adaptive regulation in response to various activity paradigms. The consensus of these findings is that the connective tissue infrastructure responds to exercise stimuli as rapidly as the myofiber complex.
With regard to physical activity and the anabolic responses of bone it appears that the response varies among different skeletal elements and across different regions of the same bone according to the recent findings of Hamrick et al . ( 15 ). Their findings on treadmill running mice for only 30 min per day suggest that the osteogenic responses of cortical bone to exercise varies significantly along the length of a bone, and more distal regions appear most likely to exhibit morphological changes when loading conditions are altered. The mechanisms for this heterogeneity have not been elucidated.
On the front of genetic and environmental factors contributing to bone mass, Suuriniemi and coworkers ( 45 ) investigated the role of PvuII polymorphism in the estrogen receptor (ER)—alpha gene concerning the activity profiles on 245-pre and early pubertal girls given that impairment of bone mass at puberty is an important risk factor for osteoporosis in later life. Their findings suggest that the PvuII polymorphism in the ER alpha gene may modulate the effect of exercise on bone mineral density at loaded sites. The heterozygotes appear to benefit most from the exercise effect; whereas, neither of the homozygote group received any significant improvement from physical activity. The findings further suggest that physical activity may hide the genetic effect on bone, e.g. , one may compensate one’s less favorable Pp genotype by increasing physical activity at early puberty. It would be interesting to determine in future research whether these exercise- induced effects are occurring via epigenetic reprogramming.
The Role of Progenitor (satellite) Cells in Muscle Adaptation
Skeletal muscle fibers (cells) are unique in that they are multinucleated and also maintain satellite cell pools in the basal lamina. Whether myonuclear addition from the satellite cell pool is a prerequisite for marked skeletal muscle fiber enlargement to occur in response to loading stimuli is the subject of ongoing inquiries in the muscle biology field. Marcus Bamman and his colleagues ( 38 ) addressed this topic by using cluster analyses of 66 subjects that underwent a rigorous quadriceps resistance exercise training program. The subjects were subsequently classified following training into 3 groups of fiber enlargement: 1) extreme responders; 2) moderate responders, and 3) nonresponders. Extreme responders had more nuclei per fiber prior to training and showed the greatest level of satellite cell expansion and incorporation into the enlarged myofibers as compared to both the moderate and non responders. These observations provide strong evidence that myonuclear proliferation/differentiation is a prerequisite for load-induced fiber enlargement in human muscle. These findings on human muscle essentially corroborate previous studies on rodent skeletal muscle that were overloaded for long duration following irradiated to prevent satellite cell proliferation/differentiation. In that study irradiation prevented the marked hypertrophy that was observed in non-irradiated muscle as well as the incorporation of satellite cells in the muscle’s nuclear domain ( 1 ). Moreover there is additional evidence that injury repair processes are also dependent on satellite cell proliferation in the repair of injured/ regenerating fibers.
Exercise and Endothelial Cardiovascular Biology
The crucial role played by the endothelium (the lining cells of blood vessels) in cardiovascular biology is becoming increasingly appreciated as endothelial dysfunction appears to have detrimental consequences and long term effects. For example, endothelial injury has been implicated in atherosclerosis, thrombosis, and hypertension. During the last ten years it has become evident that endothelial progenitor cells (EPCs), released from bone marrow, may play an important role in maintaining an intact endothelial cell layer ( 33 ). Earlier reports from animal experiments suggest that circulating EPCs bind to the activated dysfunctional epithelium via specific receptors and reconstitute the endothelial cell layer by secretion of mediators of proliferation ( 39 ). Recent research also suggests that acute exercise stimulates release of EPCs in steady state strenuous exercise along with other regulatory factors such as vascular endothelial growth Factor (VEGF) and Interleukin 6. Additionally, reports by Brehm and associates ( 9 ) provide strong evidence that physical activity predisposes the mobilization and enhanced functional activity of circulating progenitor cells that may lead to improved cardiovascular function in patients with recently acquired myocardial infarct. Finally, Hagberg and associates ( 48 ) report that chronic long duration exercise training in aging male subjects demonstrated greater hyperemic forearm blood flow compared to less active subjects even though the EPC counts were not different between the two groups. Additionally, detraining of the active subjects resulted in both a large decrease in reactive forearm blood flow and circulating EPCs and VEGF receptor number. These alterations were correlated to changes in antioxidant capacity. These collective findings clearly point to the important role that exercise plays in maintain the homeostasis of the vascular endothelial system and the dynamic nature of its response to inactivity.
Epidemiological Studies on Physical Activity and Longevity
In the last decade there have been many articles published pointing to the positive impact that physical activity plays in the evolution of several degenerative diseases such as cardiovascular dysfunction, diabetes, metabolic syndrome, and osteoporosis to name a few. In fact, studies show that physical exercise is “more protective” than might be predicted on exercise-induced changes in risk factors ( 23 ). However, the critical question is whether exercise plays a positive role in extending one’s life span. In 2001, Blair and Colleagues ( 5 ) set the tone by trying to sort out whether it was physical activity per se or the level of fitness that contributed to health benefits leading to longevity, since both were linked to reducing morbidity from coronary heart disease, stroke, cardiovascular disease, certain types of cancer, and all-cause mortality. It was recommended that future studies define more precisely the shape of the dose-response gradient across activity and the level of fitness groups with a primary focus on musculoskeletal fitness relative to additional health outcomes. While ongoing research suggests that activity level is an important contributor to longevity for both males and females, only recently did new insight occur on this important topic by focusing more-so on elite athletes. Recently, Teramonto and Bungum ( 46 ) analyzed mortality and longevity of elite athletes using a variety of standardized tests. Their findings show that elite endurance (aerobic) athletes and mixed-sport (aerobic and anaerobic) athletes survive longer than the general population, indicated by lower mortality and higher longevity. Further the results point to lower cardiovascular disease as the primary factor for these lower mortality rates. On the other hand there are inconsistent results among studies on power (anaerobic) athletes. Thus, there is some truth to the term “survival of the fittest.”
To put this important issue into a broader perspective, Fraser and Shavlik ( 13 ) studied 34,192 California Seventh-Day Adventists and found that this subject pool has higher life expectancy than other white Californians by ~7.28 years, giving them the perhaps highest expectancy of any formally described population. Additional analyses attributed this life extension to diet (leaning toward more vegetarian), exercise, lower body mass index, less dependency on hormone replacement, and lack of smoking. It might turn out that in the long run it is the behavioral choices that individuals make that contribute to one’s longevity.
Biomedical Informatics
Biomedical informatics (BMI) is an expanding field that is playing an ever growing role in health care and biomedical research. BMI now encompasses sub-disciplines such as bioinformatics, imaging informatics, clinical informatics, and public health informatics ( 14 ). Indeed, electronic medical record systems (EMRs) and numerous NIH initiatives like the Clinical Translational Science Award place a heavy emphasis on biomedical informatics. A fundamental component of biomedical informatics is the so-called “ontology,” which provides a controlled vocabulary and set of terminologies that can be used to model a domain of knowledge or discourse. Currently, an exercise/physical activity/physical inactivity specific ontology does not exist. Consequently, it is our recommendation that recognized organizations in the field of exercise science like the American College of Sports Medicine take the lead in developing ontologies that will play an essential role in accelerating breakthroughs in the field of exercise science.
Moving Forward On Two Paths
Building on a solid foundation.
Based on the topics covered above, it is clear that research initiatives in the last decade were focused heavily on gene discovery, gene expression, along with their manipulation and regulation. These new areas of study were enhanced further by the emergence of the epigenetic field. New technologies blossomed and became commonly available such that it became easier to perform molecular/biochemical analyses via kits purchased off the shelf from a large variety of vendors (which, in turn, generated a lot of junk mail). Furthermore, a wide variety of high throughput analyses systems became available in many areas in the biological sciences to include genomics, proteomics, and epigenetics. These in turn generated a “mountain” of data that required advances in the bioinformatics field to design software for better analyses and integration of the large volume of data being generated. Thus, it is safe to say that the research centered around “gene expression and function” will only get bigger and better as more information is generated and integrated in different fields, including the exercise sciences. However, is this path the only way to go?
Back To the Future: The Essence of Fundamental Biochemistry
In a recent opinion/OP-ED article in the New York Times ( www.nytimes.com/2009/08/06/opinion/06watson.html?_r=1 ) Nobel Laureate, James D. Watson, provided a deep rooted perspective on the topic: “To Fight Cancer, Know the Enemy.” Watson opined that over the years since 1971, the NIH National Cancer Institute squandered the assault on fighting cancer by putting more resources into comprehensive cancer centers rather than putting needed money into basic cancer research. While the death rates for cancer have dropped over time, the cure for cancer is nowhere on the horizon.
Watson points out that a comprehensive overview of how cancer biology works did not begin to emerge until about 2000, with more extensive details about specific cancers beginning to pour forth only after the completion of the Human Genome Project in 2003. At present, while there are promising drugs in the pipeline, these “powerful attackers” may not be effective for every case and for a life long cure. Watson postulates that the time has come to turn the focus away from decoding the genetic instructions behind cancer and to a greater degree toward understanding the “chemical reactions within cancer cells.” This concept is based on the long standing discoveries of biochemists that cancer cells, in order to grow and replicate, are almost exclusively dependent on the metabolic processes of carbohydrate metabolism which, “over-drive” reactions that lead to increase glucose transportation into these rapid growing cells to fuel the signaling driving proliferation differentiation processes. Thus, Watson argues the need to return to performing studies on the biochemistry of cells to ascertain the function and mechanisms of gene products. In the authors’ view, there are potential lessons learned from the Watson opinion piece that can be translated to the exercise sciences in dealing with a number of degenerative diseases and health epidemics.
For example, we are well aware of the critical problems associated with the problem of obesity, which seems to keep growing in spite of a lot of attention by the science community. Perhaps it is time to get back to basics. This is illustrated by the unique studies recently published by Huber and associates ( 22 ). They have made the unique observation that by under nourishing (caloric restriction) pregnant rats, that the development of the fetus is imprinted with a biochemical footprint favoring the economy of energy balance. After birth the animals grow normally in the neonatal state, but as they proceed into adulthood they become obese even though they do not consume more food than their normal sibling counterparts. Also, these animals prefer exercise relative to food intake if presented with the choice; and exercise proves to be useful in preventing the development of obesity in this model. Further, the biochemical cascade of this process is much different in its biochemical mechanism as compared to normal animal littermates that were fed high fat diets and also became obese.
To put these above findings into a human context a report by Kyle and Pichard ( 24 ) involving the Dutch famine of 1944–45, involving prenatal famine due to marked food reduction in pregnant mothers resulted in significant alterations in physiological homeostasis of the offspring. These included: increases in impaired glucose tolerance, obesity, coronary heart disease, atherogenic lipid profiles, antisocial personality and other related disorders. These unique findings point to the importance of using modern tools to dissect the signaling processes and the biochemical frame work for understanding obesity and other disorders in different types of animal models and potentially in humans with different prenatal, neonatal developmental, genetic and epigenetic imprints. Furthermore, the above phenomena raises important questions for maternal fetal programming of exercise effects, e.g. , will physically active mothers have more physically active off spring? Or will such offspring have some protection against inactivity related disorders?
In Figure 1 , we present a conceptual framework of integrating the physiology/biochemistry with genomic data as an approach for better interpretation of data in exercise physiology and potential outcomes.
Some Key Themes Driving the Exercise Science Field in the Future
The following topics listed below were provided by investigators that responded to the inquiry. They are by no means the end-all of where the science should be heading.
Exercise mimetics : The controversial paper of Ron Evans et al ( 34 ) has sparked keen interest into whether there are a wide range of pharmacological agents (exercise pills) that can activate certain pathways linked to enhancing running capacity and/or muscle growth. The key question is whether exercise stimuli are essential requirements to enhancing physical fitness and improved metabolic outcomes. See the reviews of Booth and Laye on this controversial topic ( 7 ) as well as the article by Hawley and Holloszy ( 17 ), the latter of which puts exercise mimetics in proper perspective.
Studies are already unfolding to search for large numbers of single nucleotide polymorphisms (SNPs) and invariant genomic probes (IGPs) to unlock genomic variation contributing to fitness, performance, and trainability. These probing breakthroughs are made possible by both human and mouse genotyping arrays generated by collaborations between Jackson Laboratories and Affymetrix (note that the authors have no financial conflicts of interest on these technology advancements).
Reactive oxygen species : The focus will be to understand the underlying biology of these species, including their role in regulating muscle mass under different impacting loading state and as signaling molecules for organelle, organ, and organismal adaptations.
Genomics : the genomic basis of muscle function is already expanding (due to new technologies) to gain insights on athletic performance, general health, and the exercise impact on different diseases.
The muscle from inside and out : The role of myokines, cytokines, and adipokines are thought to impact both organ systems and organism homeostasis; the new emphasis should focus on mechanisms driving such synergism.
The processing of substrate fuels during acute and chronic exercise in athletic, sedentary, and obese lifestyles.
Experiments need to be designed to ascertain the mechanism(s) of cell signaling regulation when aerobic and anabolic training paradigms are simultaneously imposed on animal and human subjects.
Muscle fiber, connective tissue, bone and satellite cell integration : each of these systems is dynamic and the challenge is to understand their integrative role in responses to various mechanical stimuli.
Mechanical sensos and signaling regulators that control muscle size : this area is largely unexplored.
Discovering biomarkers for predicting exercise and altered health settings : it is accepted that there is a large variability in how humans respond to different types of training stimuli; is it possible to predict who are the responders versus non responders.
Extreme Environments : there are many challenges to frame the underlying mechanisms as to how individuals perform in stressful environments of heat, cold, hypoxia, and insufficient nutrition.
The link between exercising muscle and brain plasticity : This is possibly the key to the real quality of life in the aging population.
Exercise and disease prevention : probably the biggest challenge for impacting the health industry in the next decade and beyond.
Mechanisms regulating aging and exercise induced longevity : The real bottom line to exercise research endeavors.
In the context of the above topics, it is important to note that several of the previous possible future research topics may involve epigenetic research to answer some critical questions which could not be solved with basic genomic approaches.
Budget Trends: Are the Necessary Resources Available To Complete the Mission?—Not
In 2000, the NIH’s Operational Budget was $22 Billion (B). It increased further to $30 B by 2003 as part of the “budget doubling package” initiated previously by Congress in the late ’90s. From that point on to the present time the budget has remained flat; and with corrections for inflation, the actual operating dollars has steadily fallen in excess of 10%. This budget profile has had a marked negative effect on NIH funding for investigator initiated R0-types of grant applications. In some of the NIH Institutes the pay line percentages are approaching single digits.
In 2009 the Obama Administration, as part of the stimulation package initiative, infused $8.4 B into the NIH budget for scientific priorities in the form of Challenge Grants in Health Science Research (these grants are supposed to provide 2 yr of funding, but with no opportunity for renewal). Also, in many of the NIH Institutes there was an infusion of money into the typical R01 type of grant, which has the potential to elevate transiently the funding level for a short period time (2009 and 2010). Presently, as this article is being written, there is no assurance that the funding profile will be enhanced to a higher steady state level in real dollars beyond the 2010 budget. Also, to the authors’ knowledge, with so many applications being submitted in the Challenge grant initiative (~20,000), it is highly unlikely that many individuals in the exercise sciences field benefited from the stimulus package initiative. This is punctuated by the fact that the pay line for most of the grants was in the second to third percentile! Thus, unless there is a dedicated stimulus to the NIH budget down the road that provides a continuous increase in the operational budget that exceeds the cost of inflation with a primary target toward RO grant applications, the authors are pessimistic concerning the potential of enhancing the research mission well beyond that which has occurred up until the present time.
From our perspective, investigators working in the field of exercise science and its related fields, have made outstanding strides on many fronts as illustrated by the examples delineated in this perspective. This occurred in spite of funding limitations during the latter half of this decade. In spite of this funding fiasco, there is available an amazing database and an assortment of state-of-the-art technologies, analytical tools and sets of resources that posture the community for bigger and better things to come. However, unless appropriate stimulating packages and stable budget profiles return to viable levels, 10 yr from now the report card or progress report will not reach its true potential.
Acknowledgments
The authors are indebted to the following individuals who contributed their insights and suggestions to the composition of this article: Greg Adams, Marcas Bamman, Claude Bouchard, Vince Caiozzo, Michael Kjaer, Mark Olfert, Bente Klarlund Pedersen, Steve Roth, Michael Sawka, Stefano Schiaffino, Espen Spangenburg, Ron Terjung, Peter Wagner, William Winder.
This article was supported in part by NIH grants AR- 30348 and HL-73473
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
- 1. Adams GR, Caiozzo VJ, Haddad F, Baldwin KM. Cellular and molecular responses to increased skeletal muscle loading after irradiation. Am J Physiol Cell Physiol. 2002;283:C1182–C1195. doi: 10.1152/ajpcell.00173.2002. [ DOI ] [ PubMed ] [ Google Scholar ]
- 2. Atherton PJ, Babraj JA, Smith K, Singh J, Rennie MJ, Wackerhage H. Selective activation of AMPK-PGC-1α or PKB-TSC2-mTOR signaling can explain specific adaptive responses to endurance or resistance training-like electrical muscle stimulation. FASEB J. 2005;19:786–788. doi: 10.1096/fj.04-2179fje. [ DOI ] [ PubMed ] [ Google Scholar ]
- 3. Baar K, Wende AR, Jones TE, et al. Adaptations of skeletal muscle to exercise: rapid increase in the transcriptional coactivator PGC-1. FASEB J. 2002;16:1879–1886. doi: 10.1096/fj.02-0367com. [ DOI ] [ PubMed ] [ Google Scholar ]
- 4. Baldwin KM. Research in the exercise sciences: Where do we go from here? J Appl Physiol. 2000;88:332–336. doi: 10.1152/jappl.2000.88.1.332. [ DOI ] [ PubMed ] [ Google Scholar ]
- 5. Blair SN, Cheng Y, Holder JS. Is physical activity or physical fitness more important in defining health benefits? Med Sci Sports Exerc. 2001;33 Suppl 6:S379–S399. doi: 10.1097/00005768-200106001-00007. [ DOI ] [ PubMed ] [ Google Scholar ]
- 6. Bodine SC. mTOR Signaling and the Molecular Adaptation to Resistance Exercise. Med Sci Sports Exerc. 2006;38:1950–1957. doi: 10.1249/01.mss.0000233797.24035.35. [ DOI ] [ PubMed ] [ Google Scholar ]
- 7. Booth FW, Laye MJ. Lack of adequate appreciation of physical exercise's complexities can pre-empt appropriate design and interpretation in scientific discovery. J Physiol. 2009 doi: 10.1113/jphysiol.2009.179507. (In Press), doi: 10.1113/jphysiol.2009.179507. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 8. Bray MSHJ, Pérusse L, Rankinen T, Roth SM, Wolfarth B, Bouchard C. The Human Gene Map for Performance and Health-Related Fitness Phenotypes:The 2006–2007 Update. Med Sci Sports Exerc. 2009;41:35–73. doi: 10.1249/mss.0b013e3181844179. [ DOI ] [ PubMed ] [ Google Scholar ]
- 9. Brehm M, Picard F, Ebner P, et al. Effects of exercise training on mobilization and functional activity of blood-derived progenitor cells in patients with acute myocardial infarction. Eur J Med Res. 2009;14:393–405. doi: 10.1186/2047-783X-14-9-393. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 10. Callis TE, Deng Z, Chen J-F, Wang D-Z. Muscling Through the microRNA World. Experimental Biology and Medicine. 2008;233:131–138. doi: 10.3181/0709-MR-237. [ DOI ] [ PubMed ] [ Google Scholar ]
- 11. Collins A, Hill LE, Chandramohan Y, Whitcomb D, Droste SK, Reul JMHM. Exercise Improves Cognitive Responses to Psychological Stress through Enhancement of Epigenetic Mechanisms and Gene Expression in the Dentate Gyrus. PLoS ONE. 2009;4:e4330. doi: 10.1371/journal.pone.0004330. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 12. Favier F, Benoit H, Freyssenet D. Cellular and molecular events controlling skeletal muscle mass in response to altered use. Pflungers Archiv European J Physiol. 2008;456:587–600. doi: 10.1007/s00424-007-0423-z. [ DOI ] [ PubMed ] [ Google Scholar ]
- 13. Fraser GE, Shavlik DJ. Ten Years of Life: Is It a Matter of Choice? Arch Intern Med. 2001;161:1645–1652. doi: 10.1001/archinte.161.13.1645. [ DOI ] [ PubMed ] [ Google Scholar ]
- 14. Greenes RAMDP, Shortliffe EHMDP. Commentary: Informatics in Biomedicine and Health Care. Acad Med. 2009;84:818–820. doi: 10.1097/ACM.0b013e3181a81f94. [Editorial]. [ DOI ] [ PubMed ] [ Google Scholar ]
- 15. Hamrick M, Skedros J, Pennington C, McNeil P. Increased osteogenic response to exercise in metaphyseal versus diaphyseal cortical bone. J Musculoskelet Neuronal Interact. 2006;6:258–263. [ PubMed ] [ Google Scholar ]
- 16. Hassan A. Potential applications of RNA interference-based therapeutics in the treatment of cardiovascular disease. Recent Pat Cardiovasc Drug Discov. 2006;1:141–149. doi: 10.2174/157489006777442540. [ DOI ] [ PubMed ] [ Google Scholar ]
- 17. Hawley JA, Holloszy JO. Exercise: it's the real thing! Nutrition Reviews. 2009;67:172–178. doi: 10.1111/j.1753-4887.2009.00185.x. [ DOI ] [ PubMed ] [ Google Scholar ]
- 18. Holloszy JO. Biochemical Adaptations in Muscle. Effects of exercise on mitochondrial oxygen uptake and respiratory enzyme activity in skeletal muscle. J Biol Chem. 1967;242:2278–2282. [ PubMed ] [ Google Scholar ]
- 19. Hollozsy J. Regulation by exercise of skeletal muscle content of mitochondria and GLUT4. J Physiol Pharmacol. 2008;59 Suppl.7:5–18. [ PubMed ] [ Google Scholar ]
- 20. Hood D. Mechanisms of exercise-induced mitochondrial biogenesis in skeletal muscle. Appl Physiol Nutr Metab. 2009;34:465–472. doi: 10.1139/H09-045. [ DOI ] [ PubMed ] [ Google Scholar ]
- 21. Howlett RA, Kirkton SD, Gonzalez NC, et al. Peripheral oxygen transport and utilization in rats following continued selective breeding for endurance running capacity. J Appl Physiol. 2009;106:1819–1825. doi: 10.1152/japplphysiol.00914.2007. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 22. Huber K, Miles JL, Norman AM, Thompson NM, Davison M, Breier BH. Prenatally Induced Changes in Muscle Structure and Metabolic Function Facilitate Exercise-Induced Obesity Prevention. Endocrinology. 2009;150:4135–4144. doi: 10.1210/en.2009-0125. [ DOI ] [ PubMed ] [ Google Scholar ]
- 23. Joyner MJ, Green DJ. Excersise protects the cardiovascular system: effects beyond traditional risk factors. The Journal of Physiology. 2009 doi: 10.1113/jphysiol.2009.179432. (in press). doi: 10.1113/jphysiol.2009.179432. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 24. Kyle UG, Pichard C. The Dutch Famine of 1944–1945: a pathophysiological model of long-term consequences of wasting disease. Current Opinion in Clinical Nutrition & Metabolic Care. 2006;9:388–394. doi: 10.1097/01.mco.0000232898.74415.42. [ DOI ] [ PubMed ] [ Google Scholar ]
- 25. Leick L, Wojtaszewski JFP, Johansen ST, et al. PGC-1{alpha} is not mandatory for exercise- and training-induced adaptive gene responses in mouse skeletal muscle. Am J Physiol Endocrinol Metab. 2008;294:E463–E474. doi: 10.1152/ajpendo.00666.2007. [ DOI ] [ PubMed ] [ Google Scholar ]
- 26. Lu PY, Xie F, Woodle MC. Non-Viral Vectors for Gene Therapy, Second Edition: Part 2. Volume 54 ed. Leaf Huang M-CH, and Ernst Wagner: Academic Press; 2005. In Vivo Application of RNA Interference: From Functional Genomics to Therapeutics. Advances in Genetics; pp. 115–142. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 27. Mackey AL, Heinemeier KM, Anneli Koskinen SO, Kjaer M. Dynamic Adaptation of Tendon and Muscle Connective Tissue to Mechanical Loading. Connective Tissue Research. 2008;49:165–168. doi: 10.1080/03008200802151672. [ DOI ] [ PubMed ] [ Google Scholar ]
- 28. Malek MH, Olfert IM. Global deletion of thrombospondin-1 increases cardiac and skeletal muscle capillarity and exercise capacity in mice. Exp Physiol. 2009;94:749–760. doi: 10.1113/expphysiol.2008.045989. [ DOI ] [ PubMed ] [ Google Scholar ]
- 29. Mammucari C, Schiaffino D, Sandri M. FoxO3 and mTOR in the regulation of autophagy in skeletal muscle. Autophagy. 2008;4:524–526. doi: 10.4161/auto.5905. [ DOI ] [ PubMed ] [ Google Scholar ]
- 30. Mehler MF. Epigenetics and the nervous system. Annals of Neurology. 2008;64:602–617. doi: 10.1002/ana.21595. [ DOI ] [ PubMed ] [ Google Scholar ]
- 31. Milagro FICJ, García-Díaz DF, Goyenechea E, Paternain L, Martínez JA. High fat diet-induced obesity modifies the methylation pattern of leptin promoter in rats. J Physiol Biochem. 2009;65:1–9. doi: 10.1007/BF03165964. [ DOI ] [ PubMed ] [ Google Scholar ]
- 32. Miyazaki M, Esser KA. Cellular mechanisms regulating protein synthesis and skeletal muscle hypertrophy in animals. J Appl Physiol. 2009;106:1367–1373. doi: 10.1152/japplphysiol.91355.2008. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 33. Moebius-Winkler S, Hilberg T, Menzel K, et al. Time Dependent Mobilization of Circulating Progenitor Cells During Strenuous Exercise in Healthy Individuals. J Appl Physiol. 2009;107(6):1943–1950. doi: 10.1152/japplphysiol.00532.2009. [ DOI ] [ PubMed ] [ Google Scholar ]
- 34. Narkar VADM, Yu RT, Embler E, et al. AMPK and PPARdelta agonists are exercise mimetics. Cell. 2008;134:405–415. doi: 10.1016/j.cell.2008.06.051. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 35. Pandorf CE, Haddad F, Roy RR, Qin AX, Edgerton VR, Baldwin KM. Dynamics of Myosin Heavy Chain Gene Regulation in Slow Skeletal Muscle: Role of Natural Antisense RNA. J Biol Chem. 2006;281:38330–38342. doi: 10.1074/jbc.M607249200. [ DOI ] [ PubMed ] [ Google Scholar ]
- 36. Pandorf CE, Haddad F, Wright C, Bodell PW, Baldwin KM. Differential epigenetic modifications of histones at the myosin heavy chain genes in fast and slow skeletal muscle fibers and in response to muscle unloading. Am J Physiol Cell Physiol. 2009;297:C6–C16. doi: 10.1152/ajpcell.00075.2009. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 37. Pedersen BK, Akerstrom TCA, Nielsen AR, Fischer CP. Role of myokines in exercise and metabolism. J Appl Physiol. 2007;103:1093–1098. doi: 10.1152/japplphysiol.00080.2007. [ DOI ] [ PubMed ] [ Google Scholar ]
- 38. Petrella JK, Kim J-s, Mayhew DL, Cross JM, Bamman MM. Potent myofiber hypertrophy during resistance training in humans is associated with satellite cell-mediated myonuclear addition: a cluster analysis. J Appl Physiol. 2008;104:1736–1742. doi: 10.1152/japplphysiol.01215.2007. [ DOI ] [ PubMed ] [ Google Scholar ]
- 39. Rehman J, Li J, Orschell CM, March KL. Peripheral Blood "Endothelial Progenitor Cells" Are Derived From Monocyte/Macrophages and Secrete Angiogenic Growth Factors. Circulation. 2003;107:1164–1169. doi: 10.1161/01.cir.0000058702.69484.a0. [ DOI ] [ PubMed ] [ Google Scholar ]
- 40. Riechman SE, Balasekaran G, Roth SM, Ferrell RE. Association of interleukin-15 protein and interleukin-15 receptor genetic variation with resistance exercise training responses. J Appl Physiol. 2004;97:2214–2219. doi: 10.1152/japplphysiol.00491.2004. [ DOI ] [ PubMed ] [ Google Scholar ]
- 41. Rinaldi C, Haddad F, Bodell PW, Qin AX, Jiang W, Baldwin KM. Intergenic Bidirectional Promoter and Cooperative Regulation of the IIx and IIb MHC Genes in Fast Skeletal Muscle. Am J Physiol Regul Integr Comp Physiol. 2008;295:208–218. doi: 10.1152/ajpregu.00134.2008. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 42. Roth SM. Perspective on the future use of genomics in exercise prescription. J Appl Physiol. 2008;104:1243–1245. doi: 10.1152/japplphysiol.01000.2007. [ DOI ] [ PubMed ] [ Google Scholar ]
- 43. Sandri M, Sandri C, Gilbert A, et al. Foxo transcription factors induce the atrophy-related ubiquitin ligase atrogin-1 and cause skeletal muscle atrophy. Cell. 2004;117:399–412. doi: 10.1016/s0092-8674(04)00400-3. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 44. Saunders M, Lim L. (micro)Genomic medicine: microRNAs as therapeutics and biomarkers. RNA Biol. 2009;6:324–328. doi: 10.4161/rna.6.3.8871. [ DOI ] [ PubMed ] [ Google Scholar ]
- 45. Suuriniemi M, Mahonen A, Kovanen V, et al. Association Between Exercise and Pubertal BMD Is Modulated by Estrogen Receptor alpha Genotype. Journal of Bone and Mineral Research. 2004;19:1758–1765. doi: 10.1359/JBMR.040918. [ DOI ] [ PubMed ] [ Google Scholar ]
- 46. Teramoto M, Bungum TJ. Mortality and longevity of elite athletes. Journal of Science and Medicine in Sport. 2009 doi: 10.1016/j.jsams.2009.04.010. (In Press) doi: 10.1016/j.jsams.2009.04.010. [ DOI ] [ PubMed ] [ Google Scholar ]
- 47. Winder W, Thomson D. Cellular energy sensing and signaling by AMP-activated protein kinase. Cell Biochemistry and Biophysics. 2007;47:332–347. doi: 10.1007/s12013-007-0008-7. [ DOI ] [ PubMed ] [ Google Scholar ]
- 48. Witkowski S, Lockard MM, Jenkins NT, Obisesan TO, E.Spangenburg E, Hagberg JM. Relationship between circulating progenitor cells to vascular function and oxidative stress with long term training and short term detraining in older men. Clin Sci. 2010;118:303–311. doi: 10.1042/CS20090253. [ DOI ] [ PMC free article ] [ PubMed ] [ Google Scholar ]
- 49. Yang N, Garton F, North K. alpha-Actinin-3 and Performance. Med Sport Sci. 2009;54:88–101. doi: 10.1159/000235698. [ DOI ] [ PubMed ] [ Google Scholar ]
- View on publisher site
- PDF (154.0 KB)
- Collections
Similar articles
Cited by other articles, links to ncbi databases.
- Download .nbib .nbib
- Format: AMA APA MLA NLM
Add to Collections
IMAGES
VIDEO
COMMENTS
College students who want to write a research paper about physiology should choose one of these unique physiology research topics for college students: Talk about motor teaching in kinesiology. Pick a muscle and analyze its anatomy. Analyze the biomechanics of the hip. Discuss motor learning in kinesiology.
Strong exercise science research topics are timely and relevant. Leading researchers and sports institutions should still be discussing them at the time you are writing your research paper. The Strength and Conditioning Journal is a great place to find some of the latest activity research topics including articles on different health benefits ...
100 Physical Fitness Research Paper Topics. The field of physical fitness offers a rich landscape for research, providing numerous opportunities for students to explore various aspects of human health, exercise, and performance. This comprehensive list of physical fitness research paper topics is designed to inspire and guide health science ...
154 Exercise Physiology Research Topics: Essay Ideas. As a scientific study of life, physiology deals with the mechanism of living organisms. It primarily focuses on the physical functions of organ systems, cells, individual organs, and biomolecules. It is the study of how the body works. By integrating both physics and chemistry, it tries to ...
Going on a research journey in Kinesiology begins with the crucial step of choosing the right topic. With its diverse disciplines having human movement, exercise science, and health, selecting a compelling research topic is major Here are ten strategic steps to guide your search for a meaningful and impactful research topic in the field of Kinesiology and they are:
ACSM creates many multimedia resources on a variety of popular topics in exercise science and sports medicine that are made freely available to the public. ACSM's Resource Library From handouts to infographics, and tips to reduce high blood pressure to exercise recommendations for pregnant women, the Resource Library houses all free resources ...
Topics in Exercise Science and Kinesiology is dedicated to relaying information to the research practitioner in an open access format.. The journal publishes original research in two main practical areas: 1) the "Process of Science" (aspects surrounding scientific discovery and practice, which could include findings from investigations, novel scientific applications, or experience gained ...
Below are some detailed research topics for kinesiology PhD students, starting with biomechanics of injury prevention in sports. 1. Biomechanics of Injury Prevention in Sports. Injury prevention is a critical area in kinesiology. With the rise of high-intensity sports and physical exercise training programs, understanding the biomechanics ...
1. Write down one or two specific topics of interest to you in your discipline (e.g. in P.T., Nursing, O.T., Athletic Training, Mental Health, etc.).. Examples: In medicine, there may be discrepancies about the best practices for reducing X condition in a certain type of patients.
Abstract. This decadal perspective summarizes novel, insightful observations achieved in exercise science. The topics span genomics and gene function, epigenetics, cell signaling, epidemiological phenomena and other important areas. A future strategy is presented along two parallel, integrated paths involving: 1) a continuance of genomic ...