How COVID-19 pandemic changed my life

Table of Contents

Introduction
The COVID-19 pandemic is one of the biggest challenges that our world has ever faced. People around the globe were affected in some way by this terrible disease, whether personally or not. Amid the COVID-19 pandemic, many people felt isolated and in a state of panic. They often found themselves lacking a sense of community, confidence, and trust. The health systems in many countries were able to successfully prevent and treat people with COVID-19-related diseases while providing early intervention services to those who may not be fully aware that they are infected (Rume & Islam, 2020). Personally, this pandemic has brought numerous changes and challenges to my life. The COVID-19 pandemic affected my social, academic, and economic lifestyle positively and negatively.

Social and Academic Changes
One of the changes brought by the pandemic was economic changes that occurred very drastically (Haleem, Javaid, & Vaishya, 2020). During the pandemic, food prices started to rise, affecting the amount of money my parents could spend on goods and services. We had to reduce the food we bought as our budgets were stretched. My family also had to eliminate unhealthy food bought in bulk, such as crisps and chocolate bars. Furthermore, the pandemic made us more aware of the importance of keeping our homes clean, especially regarding cooking food. Lastly, it also made us more aware of how we talked to other people when they were ill and stayed home with them rather than being out and getting on with other things.
Furthermore, COVID-19 had a significant effect on my academic life. Immediately, measures to curb the pandemic were announced, such as closing all learning institutions in the country; my school life changed. The change began when our school implemented the online education system to ensure that we continued with our education during the lockdown period. At first, this affected me negatively because when learning was not happening in a formal environment, I struggled academically since I was not getting the face-to-face interaction with the teachers I needed. Furthermore, forcing us to attend online caused my classmates and me to feel disconnected from the knowledge being taught because we were unable to have peer participation in class. However, as the pandemic subsided, we grew accustomed to this learning mode. We realized the effects on our performance and learning satisfaction were positive, as it seemed to promote emotional and behavioral changes necessary to function in a virtual world. Students who participated in e-learning during the pandemic developed more ownership of the course requirement, increased their emotional intelligence and self-awareness, improved their communication skills, and learned to work together as a community.

If there is an area that the pandemic affected was the mental health of my family and myself. The COVID-19 pandemic caused increased anxiety, depression, and other mental health concerns that were difficult for my family and me to manage alone. Our ability to learn social resilience skills, such as self-management, was tested numerous times. One of the most visible challenges we faced was social isolation and loneliness. The multiple lockdowns made it difficult to interact with my friends and family, leading to loneliness. The changes in communication exacerbated the problem as interactions moved from face-to-face to online communication using social media and text messages. Furthermore, having family members and loved ones separated from us due to distance, unavailability of phones, and the internet created a situation of fear among us, as we did not know whether they were all right. Moreover, some people within my circle found it more challenging to communicate with friends, family, and co-workers due to poor communication skills. This was mainly attributed to anxiety or a higher risk of spreading the disease. It was also related to a poor understanding of creating and maintaining relationships during this period.
Positive Changes
In addition, this pandemic has brought some positive changes with it. First, it had been a significant catalyst for strengthening relationships and neighborhood ties. It has encouraged a sense of community because family members, neighbors, friends, and community members within my area were all working together to help each other out. Before the pandemic, everybody focused on their business, the children going to school while the older people went to work. There was not enough time to bond with each other. Well, the pandemic changed that, something that has continued until now that everything is returning to normal. In our home, it strengthened the relationship between myself and my siblings and parents. This is because we started spending more time together as a family, which enhanced our sense of understanding of ourselves.

The pandemic has been a challenging time for many people. I can confidently state that it was a significant and potentially unprecedented change in our daily life. By changing how we do things and relate with our family and friends, the pandemic has shaped our future life experiences and shown that during crises, we can come together and make a difference in each other’s lives. Therefore, I embrace wholesomely the changes brought by the COVID-19 pandemic in my life.
- Haleem, A., Javaid, M., & Vaishya, R. (2020). Effects of COVID-19 pandemic in daily life. Current medicine research and practice , 10 (2), 78.
- Rume, T., & Islam, S. D. U. (2020). Environmental effects of COVID-19 pandemic and potential strategies of sustainability. Heliyon , 6 (9), e04965.
- ☠️ Assisted Suicide
- Affordable Care Act
- Breast Cancer
- Genetic Engineering

- Newsletters
Site search
- Israel-Hamas war
- 2024 election
- TikTok’s fate
- Supreme Court
- Winter warming
- All explainers
- Future Perfect
Filed under:
Read these 12 moving essays about life during coronavirus
Artists, novelists, critics, and essayists are writing the first draft of history.
Share this story
- Share this on Facebook
- Share this on Twitter
- Share this on Reddit
- Share All sharing options
Share All sharing options for: Read these 12 moving essays about life during coronavirus
/cdn.vox-cdn.com/uploads/chorus_image/image/66606035/1207638131.jpg.0.jpg)
The world is grappling with an invisible, deadly enemy, trying to understand how to live with the threat posed by a virus . For some writers, the only way forward is to put pen to paper, trying to conceptualize and document what it feels like to continue living as countries are under lockdown and regular life seems to have ground to a halt.
So as the coronavirus pandemic has stretched around the world, it’s sparked a crop of diary entries and essays that describe how life has changed. Novelists, critics, artists, and journalists have put words to the feelings many are experiencing. The result is a first draft of how we’ll someday remember this time, filled with uncertainty and pain and fear as well as small moments of hope and humanity.
At the New York Review of Books, Ali Bhutto writes that in Karachi, Pakistan, the government-imposed curfew due to the virus is “eerily reminiscent of past military clampdowns”:
Beneath the quiet calm lies a sense that society has been unhinged and that the usual rules no longer apply. Small groups of pedestrians look on from the shadows, like an audience watching a spectacle slowly unfolding. People pause on street corners and in the shade of trees, under the watchful gaze of the paramilitary forces and the police.
His essay concludes with the sobering note that “in the minds of many, Covid-19 is just another life-threatening hazard in a city that stumbles from one crisis to another.”
Writing from Chattanooga, novelist Jamie Quatro documents the mixed ways her neighbors have been responding to the threat, and the frustration of conflicting direction, or no direction at all, from local, state, and federal leaders:
Whiplash, trying to keep up with who’s ordering what. We’re already experiencing enough chaos without this back-and-forth. Why didn’t the federal government issue a nationwide shelter-in-place at the get-go, the way other countries did? What happens when one state’s shelter-in-place ends, while others continue? Do states still under quarantine close their borders? We are still one nation, not fifty individual countries. Right?
Award-winning photojournalist Alessio Mamo, quarantined with his partner Marta in Sicily after she tested positive for the virus, accompanies his photographs in the Guardian of their confinement with a reflection on being confined :
The doctors asked me to take a second test, but again I tested negative. Perhaps I’m immune? The days dragged on in my apartment, in black and white, like my photos. Sometimes we tried to smile, imagining that I was asymptomatic, because I was the virus. Our smiles seemed to bring good news. My mother left hospital, but I won’t be able to see her for weeks. Marta started breathing well again, and so did I. I would have liked to photograph my country in the midst of this emergency, the battles that the doctors wage on the frontline, the hospitals pushed to their limits, Italy on its knees fighting an invisible enemy. That enemy, a day in March, knocked on my door instead.
In the New York Times Magazine, deputy editor Jessica Lustig writes with devastating clarity about her family’s life in Brooklyn while her husband battled the virus, weeks before most people began taking the threat seriously:
At the door of the clinic, we stand looking out at two older women chatting outside the doorway, oblivious. Do I wave them away? Call out that they should get far away, go home, wash their hands, stay inside? Instead we just stand there, awkwardly, until they move on. Only then do we step outside to begin the long three-block walk home. I point out the early magnolia, the forsythia. T says he is cold. The untrimmed hairs on his neck, under his beard, are white. The few people walking past us on the sidewalk don’t know that we are visitors from the future. A vision, a premonition, a walking visitation. This will be them: Either T, in the mask, or — if they’re lucky — me, tending to him.
Essayist Leslie Jamison writes in the New York Review of Books about being shut away alone in her New York City apartment with her 2-year-old daughter since she became sick:
The virus. Its sinewy, intimate name. What does it feel like in my body today? Shivering under blankets. A hot itch behind the eyes. Three sweatshirts in the middle of the day. My daughter trying to pull another blanket over my body with her tiny arms. An ache in the muscles that somehow makes it hard to lie still. This loss of taste has become a kind of sensory quarantine. It’s as if the quarantine keeps inching closer and closer to my insides. First I lost the touch of other bodies; then I lost the air; now I’ve lost the taste of bananas. Nothing about any of these losses is particularly unique. I’ve made a schedule so I won’t go insane with the toddler. Five days ago, I wrote Walk/Adventure! on it, next to a cut-out illustration of a tiger—as if we’d see tigers on our walks. It was good to keep possibility alive.
At Literary Hub, novelist Heidi Pitlor writes about the elastic nature of time during her family’s quarantine in Massachusetts:
During a shutdown, the things that mark our days—commuting to work, sending our kids to school, having a drink with friends—vanish and time takes on a flat, seamless quality. Without some self-imposed structure, it’s easy to feel a little untethered. A friend recently posted on Facebook: “For those who have lost track, today is Blursday the fortyteenth of Maprilay.” ... Giving shape to time is especially important now, when the future is so shapeless. We do not know whether the virus will continue to rage for weeks or months or, lord help us, on and off for years. We do not know when we will feel safe again. And so many of us, minus those who are gifted at compartmentalization or denial, remain largely captive to fear. We may stay this way if we do not create at least the illusion of movement in our lives, our long days spent with ourselves or partners or families.
Novelist Lauren Groff writes at the New York Review of Books about trying to escape the prison of her fears while sequestered at home in Gainesville, Florida:
Some people have imaginations sparked only by what they can see; I blame this blinkered empiricism for the parks overwhelmed with people, the bars, until a few nights ago, thickly thronged. My imagination is the opposite. I fear everything invisible to me. From the enclosure of my house, I am afraid of the suffering that isn’t present before me, the people running out of money and food or drowning in the fluid in their lungs, the deaths of health-care workers now growing ill while performing their duties. I fear the federal government, which the right wing has so—intentionally—weakened that not only is it insufficient to help its people, it is actively standing in help’s way. I fear we won’t sufficiently punish the right. I fear leaving the house and spreading the disease. I fear what this time of fear is doing to my children, their imaginations, and their souls.
At ArtForum , Berlin-based critic and writer Kristian Vistrup Madsen reflects on martinis, melancholia, and Finnish artist Jaakko Pallasvuo’s 2018 graphic novel Retreat , in which three young people exile themselves in the woods:
In melancholia, the shape of what is ending, and its temporality, is sprawling and incomprehensible. The ambivalence makes it hard to bear. The world of Retreat is rendered in lush pink and purple watercolors, which dissolve into wild and messy abstractions. In apocalypse, the divisions established in genesis bleed back out. My own Corona-retreat is similarly soft, color-field like, each day a blurred succession of quarantinis, YouTube–yoga, and televized press conferences. As restrictions mount, so does abstraction. For now, I’m still rooting for love to save the world.
At the Paris Review , Matt Levin writes about reading Virginia Woolf’s novel The Waves during quarantine:
A retreat, a quarantine, a sickness—they simultaneously distort and clarify, curtail and expand. It is an ideal state in which to read literature with a reputation for difficulty and inaccessibility, those hermetic books shorn of the handholds of conventional plot or characterization or description. A novel like Virginia Woolf’s The Waves is perfect for the state of interiority induced by quarantine—a story of three men and three women, meeting after the death of a mutual friend, told entirely in the overlapping internal monologues of the six, interspersed only with sections of pure, achingly beautiful descriptions of the natural world, a day’s procession and recession of light and waves. The novel is, in my mind’s eye, a perfectly spherical object. It is translucent and shimmering and infinitely fragile, prone to shatter at the slightest disturbance. It is not a book that can be read in snatches on the subway—it demands total absorption. Though it revels in a stark emotional nakedness, the book remains aloof, remote in its own deep self-absorption.
In an essay for the Financial Times, novelist Arundhati Roy writes with anger about Indian Prime Minister Narendra Modi’s anemic response to the threat, but also offers a glimmer of hope for the future:
Historically, pandemics have forced humans to break with the past and imagine their world anew. This one is no different. It is a portal, a gateway between one world and the next. We can choose to walk through it, dragging the carcasses of our prejudice and hatred, our avarice, our data banks and dead ideas, our dead rivers and smoky skies behind us. Or we can walk through lightly, with little luggage, ready to imagine another world. And ready to fight for it.
From Boston, Nora Caplan-Bricker writes in The Point about the strange contraction of space under quarantine, in which a friend in Beirut is as close as the one around the corner in the same city:
It’s a nice illusion—nice to feel like we’re in it together, even if my real world has shrunk to one person, my husband, who sits with his laptop in the other room. It’s nice in the same way as reading those essays that reframe social distancing as solidarity. “We must begin to see the negative space as clearly as the positive, to know what we don’t do is also brilliant and full of love,” the poet Anne Boyer wrote on March 10th, the day that Massachusetts declared a state of emergency. If you squint, you could almost make sense of this quarantine as an effort to flatten, along with the curve, the distinctions we make between our bonds with others. Right now, I care for my neighbor in the same way I demonstrate love for my mother: in all instances, I stay away. And in moments this month, I have loved strangers with an intensity that is new to me. On March 14th, the Saturday night after the end of life as we knew it, I went out with my dog and found the street silent: no lines for restaurants, no children on bicycles, no couples strolling with little cups of ice cream. It had taken the combined will of thousands of people to deliver such a sudden and complete emptiness. I felt so grateful, and so bereft.
And on his own website, musician and artist David Byrne writes about rediscovering the value of working for collective good , saying that “what is happening now is an opportunity to learn how to change our behavior”:
In emergencies, citizens can suddenly cooperate and collaborate. Change can happen. We’re going to need to work together as the effects of climate change ramp up. In order for capitalism to survive in any form, we will have to be a little more socialist. Here is an opportunity for us to see things differently — to see that we really are all connected — and adjust our behavior accordingly. Are we willing to do this? Is this moment an opportunity to see how truly interdependent we all are? To live in a world that is different and better than the one we live in now? We might be too far down the road to test every asymptomatic person, but a change in our mindsets, in how we view our neighbors, could lay the groundwork for the collective action we’ll need to deal with other global crises. The time to see how connected we all are is now.
The portrait these writers paint of a world under quarantine is multifaceted. Our worlds have contracted to the confines of our homes, and yet in some ways we’re more connected than ever to one another. We feel fear and boredom, anger and gratitude, frustration and strange peace. Uncertainty drives us to find metaphors and images that will let us wrap our minds around what is happening.
Yet there’s no single “what” that is happening. Everyone is contending with the pandemic and its effects from different places and in different ways. Reading others’ experiences — even the most frightening ones — can help alleviate the loneliness and dread, a little, and remind us that what we’re going through is both unique and shared by all.
Will you help keep Vox free for all?
At Vox, we believe that clarity is power, and that power shouldn’t only be available to those who can afford to pay. That’s why we keep our work free. Millions rely on Vox’s clear, high-quality journalism to understand the forces shaping today’s world. Support our mission and help keep Vox free for all by making a financial contribution to Vox today.
We accept credit card, Apple Pay, and Google Pay. You can also contribute via
Next Up In Culture
Sign up for the newsletter today, explained.
Understand the world with a daily explainer plus the most compelling stories of the day.
Thanks for signing up!
Check your inbox for a welcome email.
Oops. Something went wrong. Please enter a valid email and try again.

3 reasons why Kate Middleton’s royal scandal got so out of control

Fani Willis’s Trump prosecution can move forward — if she drops her ex from the case

Why abortion politics might not carry Democrats again in 2024

This AI says it has feelings. It’s wrong. Right?

How to think about Boeing’s recent safety issues

How the world has radically cut child deaths, in one chart
Two Years In: How the Pandemic Changed Our Lives
From remote work to major life developments, the COVID-19 era left its mark on Duke staff and faculty

- Share this story on facebook
- Share this story on twitter
- Share this story on reddit
- Share this story on linkedin
- Get this story's permalink
- Print this story
Two years ago this week, the novel coronavirus fully took hold in the United States. While it had been in the country earlier, the second week of March 2020 was when cases spiked, and soon after, Duke University President Vincent E. Price announced in an “urgent message” that faculty and staff who could work from home should do so.
Masking and social distancing policies became the norm while businesses, schools and offices went quiet.
As some safety measures ease , COVID-19 has infected nearly 80 million Americans and left nearly 970,000 dead. As the pandemic raged with variants, education, research and health care continued across Duke University and Duke University Health System at a high level.
And many of us are forever changed.
“I think we, as a people, are different,” said Duke Associate Professor of Medicine Jon Bae, a co-convener for the mental and emotional well-being portion of Healthy Duke. “In the last two years, people have learned different ways of working, different ways of living and different ways to take appreciation for things.”
Jon Boylan is one of those.

The past two years have drawn Boylan closer to his wife, Katie, a steadying influence during uncertain times. But starting a family against the backdrop of a global pandemic has given him a deeper respect for how forces outside of our control can alter plans.
“I wasn’t one of those people who had time to learn how to bake bread or anything,” Boylan said. “But I think in terms of personal growth, a lot happened.”
We caught up with some Duke colleagues to hear how their lives are different two years into the pandemic.
Committing to Self-Care

“For me, I thought, ‘How do I have a rich, full life amid all of this and keep a positive attitude?’” Thomas said.
She decided that she needed a goal that she could work toward until the world opened up. Already with a long list of outdoors adventures under her belt, Thomas decided to plan a summer 2021 trip to Nepal to hike the summit of the 21,247-foot Mera Peak.
For the next several months, Thomas began running, working out at a socially distanced gym, and incorporating as many walks as possible into her day. While the trip to Nepal was the goal, the exercise to prepare for it became a central piece of her self-care routine.
“I just love being outside, it’s very restorative,” Thomas said. “And I like physical challenges, I get the rush of endorphins from that. So putting those two things together just helps me out mentally. Even just a short walk can help me focus.”
Eventually, travel complications required Thomas to postpone the trip to Nepal. Instead, she flew to Spain and, over three weeks in September and October of 2021, she hiked 335 miles on the Camino de Santiago pilgrim trail.
“It was basically like a walking meditation for three weeks,” said Thomas, who is now exercising with an eye toward a 2023 Nepal trip. “It’s really an incredible experience.”
Defining Your Purpose

But she said COVID-19 tested everyone’s resolve.
“You just don’t know how you’re going to react to something until you’re in it,” Casey said.
In March 2020, Casey was the clinical team lead for Duke Raleigh’s ICU, a managerial role with less hands-on patient care. But it wasn’t far into the pandemic before Casey’s desire to help patients led her to return to a clinical nurse role.
There, she saw the virus’ danger up close. At one point in the summer of 2020, 13 of the 15 beds in the ICU were occupied by COVID-19 patients on ventilators. With no visitors allowed for COVID-19 patients, Casey witnessed several wrenching goodbyes said over cellphone.
Her challenges didn’t end when she left work. With four children and a husband who’s a police officer in Durham, at home, Casey faced stress from home schooling and a spouse also on COVID-19’s front lines.
While many ICU nurses ask to be transferred to different units due to the emotional strain, Casey was inspired by seeing colleagues bravely push forward, giving comfort and dignity to patients facing dire situations. She also said that, as the pandemic wore on, the bond between ICU nurses grew stronger.
As hard as these past two years have been, Casey, who still serves in the ICU and recently began working toward an Acute Care Nurse Practitioner certificate through the Duke University School of Nursing , said the pandemic experience has only deepened her connection to her work.
“We all faced this as a challenge, personally, emotionally and professionally, and hopefully learned to grow through it and be better if this ever happens again,” Casey said.
Taking Charge of Physical Health

After the pandemic required many Duke staff and faculty members to work remotely , sending Carbuccia from working in the bustling Smith Warehouse to his Mebane home, the IT Analyst with Duke’s Office of Information Technology found himself making healthier choices without even thinking.
Instead of eating lunch out or grabbing meals from events in his on-campus workspace, Carbuccia found himself eating homemade breakfasts, lunches and dinners. Scrambled eggs with vegetables, or simply prepared salmon filets are some of current favorites.
And without a commute, he has time for walks around his neighborhood before and after work.
Carbuccia saw the result of these changes a few months into the pandemic when he stepped on the scale and saw that he’d lost 26 pounds.
“When I stepped on the scale, I said, ‘Holy Moses! I lost a lot of weight, and I wasn’t even planning to!’” Carbuccia said.
A Better Mental Space

And each day also involved a roughly 30-minute commute along I-85 to her home in Graham, where the heavy traffic made her feel especially anxious, leaving her tense when she arrived at work or home.
But the past two years saw her work go fully remote, and now a move to a hybrid arrangement featuring one day of on-site each week. She cherishes the time she can spend working from home, often with her two dogs – Marx, a Boston Terrier, and Duke, a rescue – lounging at her feet.
“Working at home, I feel like my mental health is in a better place,” said Herrera, a wife and mother of three.
Herrera isn’t alone in her appreciation of remote work. According to a Pew Research Center report from February 2022, approximately six in 10 workers who can do their jobs from home are working remotely most or all of the time.
Herrera said her hybrid schedule leaves her feeling mentally fresh when she begins her workday and better able to transition between work and personal life.
“I’m happier,” Herrera said. “I’m more at ease.”
Learning on the Fly

“Even though some of us had experience working remotely, it was still new,” said Roberts, who’s worked at Duke for nearly a decade. “Regardless of how much experience you had, I don’t think we were mentally or technologically ready for that quick of a transition.”
Roberts recalls PRMO leaders moving quickly to get desktops, monitors, laptops, cameras and headsets in the hands of team members. She also recalls many of her colleagues working diligently to familiarize themselves with new tools and programs, such as the collaboration platform Jabber, that were different from what was used in the PRMO offices on South Alston Avenue in Durham.
Roberts and her colleagues also had to learn how to collaborate with one another when communication came by email and chat messages instead of a quick face-to-face conversation.
Working each day from her home in Franklinton, Roberts continues to help Duke Health patients with billing concerns. She’s part of a large team that gelled amid the pandemic and kept the pace of customer support high.
With PRMO keeping colleagues connected with department meetings and team-building Zoom events, Roberts said these past two years have given her a new appreciation of the resilience of her colleagues.
“It made me proud because nobody skipped a beat,” Roberts said. “Everybody took accountability. While some of our thinking and the logic behind how we normally do things had to change, I’m proud that it was still a really seamless transition for us.”
Finding Flexibility

“This is something that would have never happened before the pandemic,” said Atkinson, a regulatory coordinator with the Duke Department of Surgery .
Like many administrators in Duke’s research areas, Atkinson has been working fully remote since the pandemic began, trading in her fourth-floor workspace in Erwin Terrace for a spot at home. The change reshaped Atkinson’s day-to-day routine in a drastic way, ridding her of a commute that ate up two hours each day.
Now, with more time to spend with her son, West, born before the pandemic, and her 10-month-old daughter, Iris, Atkinson, who has worked for Duke for nearly seven years, has the flexibility that allows her to feel rooted. And with more balance, she hopes to let the roots of her family, as well as the cucumbers, tomatoes and peppers that will be in the ground soon, grow strong.
“I’ve attempted a very small garden each year, but we have a very shady lot,” Atkinson said. “But this year, we’re putting it in the front, where we get a lot of sun, and West is helping me, so it’s going to work.”
A World of Change

In late 2019, she met Neil Gallagher at a party and hit it off. The pair dated for the next few months and, when the pandemic forced everyone to limit contact with others, they decided to keep each other in their quarantine bubble.
“It was one of those easy connections where we were really comfortable with each other,” said Meyer, who shared the story of her mental health journey with Working@Duke just before the coronavirus outbreak.
Over the next several months, the pair grew closer and, by the end of 2020, they’d begun talking about getting engaged and starting a family. Those plans hit warp speed when they found out Meyer was pregnant in early 2021. Not long after, they were engaged and later married in a small ceremony in Raleigh in July of last year.
And over a few hectic days in early October, the pair closed on a house together in Raleigh and Meyer gave birth to a healthy baby girl named Maggie.
Now in a very different spot in life from where she was when the pandemic began, Meyer said she greets each day with a new feeling of purpose and strong sense of gratitude.
“I think my husband and I have been keenly aware of how odd it’s been and how many blessing we’ve had at a time when life has been really hard for a lot of people,” Meyer said.
How has the pandemic changed your life? Send us your story and photographs through our story idea form or write [email protected] .
Follow Working@Duke on Twitter and Facebook .
Link to this page
Copy and paste the URL below to share this page.
I Thought We’d Learned Nothing From the Pandemic. I Wasn’t Seeing the Full Picture

M y first home had a back door that opened to a concrete patio with a giant crack down the middle. When my sister and I played, I made sure to stay on the same side of the divide as her, just in case. The 1988 film The Land Before Time was one of the first movies I ever saw, and the image of the earth splintering into pieces planted its roots in my brain. I believed that, even in my own backyard, I could easily become the tiny Triceratops separated from her family, on the other side of the chasm, as everything crumbled into chaos.
Some 30 years later, I marvel at the eerie, unexpected ways that cartoonish nightmare came to life – not just for me and my family, but for all of us. The landscape was already covered in fissures well before COVID-19 made its way across the planet, but the pandemic applied pressure, and the cracks broke wide open, separating us from each other physically and ideologically. Under the weight of the crisis, we scattered and landed on such different patches of earth we could barely see each other’s faces, even when we squinted. We disagreed viciously with each other, about how to respond, but also about what was true.
Recently, someone asked me if we’ve learned anything from the pandemic, and my first thought was a flat no. Nothing. There was a time when I thought it would be the very thing to draw us together and catapult us – as a capital “S” Society – into a kinder future. It’s surreal to remember those early days when people rallied together, sewing masks for health care workers during critical shortages and gathering on balconies in cities from Dallas to New York City to clap and sing songs like “Yellow Submarine.” It felt like a giant lightning bolt shot across the sky, and for one breath, we all saw something that had been hidden in the dark – the inherent vulnerability in being human or maybe our inescapable connectedness .
More from TIME
Read More: The Family Time the Pandemic Stole
But it turns out, it was just a flash. The goodwill vanished as quickly as it appeared. A couple of years later, people feel lied to, abandoned, and all on their own. I’ve felt my own curiosity shrinking, my willingness to reach out waning , my ability to keep my hands open dwindling. I look out across the landscape and see selfishness and rage, burnt earth and so many dead bodies. Game over. We lost. And if we’ve already lost, why try?
Still, the question kept nagging me. I wondered, am I seeing the full picture? What happens when we focus not on the collective society but at one face, one story at a time? I’m not asking for a bow to minimize the suffering – a pretty flourish to put on top and make the whole thing “worth it.” Yuck. That’s not what we need. But I wondered about deep, quiet growth. The kind we feel in our bodies, relationships, homes, places of work, neighborhoods.
Like a walkie-talkie message sent to my allies on the ground, I posted a call on my Instagram. What do you see? What do you hear? What feels possible? Is there life out here? Sprouting up among the rubble? I heard human voices calling back – reports of life, personal and specific. I heard one story at a time – stories of grief and distrust, fury and disappointment. Also gratitude. Discovery. Determination.
Among the most prevalent were the stories of self-revelation. Almost as if machines were given the chance to live as humans, people described blossoming into fuller selves. They listened to their bodies’ cues, recognized their desires and comforts, tuned into their gut instincts, and honored the intuition they hadn’t realized belonged to them. Alex, a writer and fellow disabled parent, found the freedom to explore a fuller version of herself in the privacy the pandemic provided. “The way I dress, the way I love, and the way I carry myself have both shrunk and expanded,” she shared. “I don’t love myself very well with an audience.” Without the daily ritual of trying to pass as “normal” in public, Tamar, a queer mom in the Netherlands, realized she’s autistic. “I think the pandemic helped me to recognize the mask,” she wrote. “Not that unmasking is easy now. But at least I know it’s there.” In a time of widespread suffering that none of us could solve on our own, many tended to our internal wounds and misalignments, large and small, and found clarity.
Read More: A Tool for Staying Grounded in This Era of Constant Uncertainty
I wonder if this flourishing of self-awareness is at least partially responsible for the life alterations people pursued. The pandemic broke open our personal notions of work and pushed us to reevaluate things like time and money. Lucy, a disabled writer in the U.K., made the hard decision to leave her job as a journalist covering Westminster to write freelance about her beloved disability community. “This work feels important in a way nothing else has ever felt,” she wrote. “I don’t think I’d have realized this was what I should be doing without the pandemic.” And she wasn’t alone – many people changed jobs , moved, learned new skills and hobbies, became politically engaged.
Perhaps more than any other shifts, people described a significant reassessment of their relationships. They set boundaries, said no, had challenging conversations. They also reconnected, fell in love, and learned to trust. Jeanne, a quilter in Indiana, got to know relatives she wouldn’t have connected with if lockdowns hadn’t prompted weekly family Zooms. “We are all over the map as regards to our belief systems,” she emphasized, “but it is possible to love people you don’t see eye to eye with on every issue.” Anna, an anti-violence advocate in Maine, learned she could trust her new marriage: “Life was not a honeymoon. But we still chose to turn to each other with kindness and curiosity.” So many bonds forged and broken, strengthened and strained.
Instead of relying on default relationships or institutional structures, widespread recalibrations allowed for going off script and fortifying smaller communities. Mara from Idyllwild, Calif., described the tangible plan for care enacted in her town. “We started a mutual-aid group at the beginning of the pandemic,” she wrote, “and it grew so quickly before we knew it we were feeding 400 of the 4000 residents.” She didn’t pretend the conditions were ideal. In fact, she expressed immense frustration with our collective response to the pandemic. Even so, the local group rallied and continues to offer assistance to their community with help from donations and volunteers (many of whom were originally on the receiving end of support). “I’ve learned that people thrive when they feel their connection to others,” she wrote. Clare, a teacher from the U.K., voiced similar conviction as she described a giant scarf she’s woven out of ribbons, each representing a single person. The scarf is “a collection of stories, moments and wisdom we are sharing with each other,” she wrote. It now stretches well over 1,000 feet.
A few hours into reading the comments, I lay back on my bed, phone held against my chest. The room was quiet, but my internal world was lighting up with firefly flickers. What felt different? Surely part of it was receiving personal accounts of deep-rooted growth. And also, there was something to the mere act of asking and listening. Maybe it connected me to humans before battle cries. Maybe it was the chance to be in conversation with others who were also trying to understand – what is happening to us? Underneath it all, an undeniable thread remained; I saw people peering into the mess and narrating their findings onto the shared frequency. Every comment was like a flare into the sky. I’m here! And if the sky is full of flares, we aren’t alone.
I recognized my own pandemic discoveries – some minor, others massive. Like washing off thick eyeliner and mascara every night is more effort than it’s worth; I can transform the mundane into the magical with a bedsheet, a movie projector, and twinkle lights; my paralyzed body can mother an infant in ways I’d never seen modeled for me. I remembered disappointing, bewildering conversations within my own family of origin and our imperfect attempts to remain close while also seeing things so differently. I realized that every time I get the weekly invite to my virtual “Find the Mumsies” call, with a tiny group of moms living hundreds of miles apart, I’m being welcomed into a pocket of unexpected community. Even though we’ve never been in one room all together, I’ve felt an uncommon kind of solace in their now-familiar faces.
Hope is a slippery thing. I desperately want to hold onto it, but everywhere I look there are real, weighty reasons to despair. The pandemic marks a stretch on the timeline that tangles with a teetering democracy, a deteriorating planet , the loss of human rights that once felt unshakable . When the world is falling apart Land Before Time style, it can feel trite, sniffing out the beauty – useless, firing off flares to anyone looking for signs of life. But, while I’m under no delusions that if we just keep trudging forward we’ll find our own oasis of waterfalls and grassy meadows glistening in the sunshine beneath a heavenly chorus, I wonder if trivializing small acts of beauty, connection, and hope actually cuts us off from resources essential to our survival. The group of abandoned dinosaurs were keeping each other alive and making each other laugh well before they made it to their fantasy ending.
Read More: How Ice Cream Became My Own Personal Act of Resistance
After the monarch butterfly went on the endangered-species list, my friend and fellow writer Hannah Soyer sent me wildflower seeds to plant in my yard. A simple act of big hope – that I will actually plant them, that they will grow, that a monarch butterfly will receive nourishment from whatever blossoms are able to push their way through the dirt. There are so many ways that could fail. But maybe the outcome wasn’t exactly the point. Maybe hope is the dogged insistence – the stubborn defiance – to continue cultivating moments of beauty regardless. There is value in the planting apart from the harvest.
I can’t point out a single collective lesson from the pandemic. It’s hard to see any great “we.” Still, I see the faces in my moms’ group, making pancakes for their kids and popping on between strings of meetings while we try to figure out how to raise these small people in this chaotic world. I think of my friends on Instagram tending to the selves they discovered when no one was watching and the scarf of ribbons stretching the length of more than three football fields. I remember my family of three, holding hands on the way up the ramp to the library. These bits of growth and rings of support might not be loud or right on the surface, but that’s not the same thing as nothing. If we only cared about the bottom-line defeats or sweeping successes of the big picture, we’d never plant flowers at all.
More Must-Reads From TIME
- Why We're Spending So Much Money Now
- The Fight to Free Evan Gershkovich
- Meet the 2024 Women of the Year
- John Kerry's Next Move
- The Quiet Work Trees Do for the Planet
- Breaker Sunny Choi Is Heading to Paris
- Column: The Internet Made Romantic Betrayal Even More Devastating
- Want Weekly Recs on What to Watch, Read, and More? Sign Up for Worth Your Time
Contact us at [email protected]
You May Also Like
Read our research on: TikTok | Podcasts | Election 2024
Regions & Countries

In Their Own Words, Americans Describe the Struggles and Silver Linings of the COVID-19 Pandemic
The outbreak has dramatically changed americans’ lives and relationships over the past year. we asked people to tell us about their experiences – good and bad – in living through this moment in history..
Pew Research Center has been asking survey questions over the past year about Americans’ views and reactions to the COVID-19 pandemic. In August, we gave the public a chance to tell us in their own words how the pandemic has affected them in their personal lives. We wanted to let them tell us how their lives have become more difficult or challenging, and we also asked about any unexpectedly positive events that might have happened during that time.
The vast majority of Americans (89%) mentioned at least one negative change in their own lives, while a smaller share (though still a 73% majority) mentioned at least one unexpected upside. Most have experienced these negative impacts and silver linings simultaneously: Two-thirds (67%) of Americans mentioned at least one negative and at least one positive change since the pandemic began.
For this analysis, we surveyed 9,220 U.S. adults between Aug. 31-Sept. 7, 2020. Everyone who completed the survey is a member of Pew Research Center’s American Trends Panel (ATP), an online survey panel that is recruited through national, random sampling of residential addresses. This way nearly all U.S. adults have a chance of selection. The survey is weighted to be representative of the U.S. adult population by gender, race, ethnicity, partisan affiliation, education and other categories. Read more about the ATP’s methodology .
Respondents to the survey were asked to describe in their own words how their lives have been difficult or challenging since the beginning of the coronavirus outbreak, and to describe any positive aspects of the situation they have personally experienced as well. Overall, 84% of respondents provided an answer to one or both of the questions. The Center then categorized a random sample of 4,071 of their answers using a combination of in-house human coders, Amazon’s Mechanical Turk service and keyword-based pattern matching. The full methodology and questions used in this analysis can be found here.
In many ways, the negatives clearly outweigh the positives – an unsurprising reaction to a pandemic that had killed more than 180,000 Americans at the time the survey was conducted. Across every major aspect of life mentioned in these responses, a larger share mentioned a negative impact than mentioned an unexpected upside. Americans also described the negative aspects of the pandemic in greater detail: On average, negative responses were longer than positive ones (27 vs. 19 words). But for all the difficulties and challenges of the pandemic, a majority of Americans were able to think of at least one silver lining.
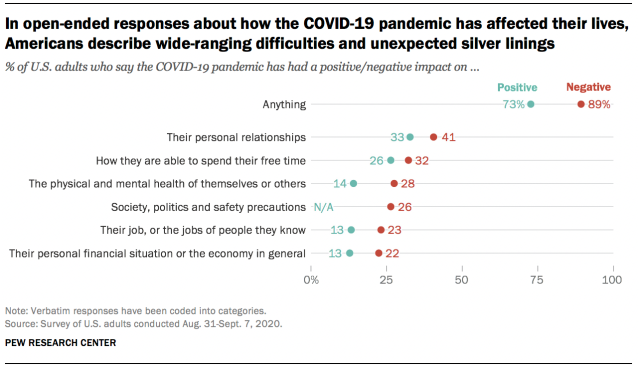
Both the negative and positive impacts described in these responses cover many aspects of life, none of which were mentioned by a majority of Americans. Instead, the responses reveal a pandemic that has affected Americans’ lives in a variety of ways, of which there is no “typical” experience. Indeed, not all groups seem to have experienced the pandemic equally. For instance, younger and more educated Americans were more likely to mention silver linings, while women were more likely than men to mention challenges or difficulties.
Here are some direct quotes that reveal how Americans are processing the new reality that has upended life across the country.
Sign up for our weekly newsletter
Fresh data delivered Saturday mornings
About Pew Research Center Pew Research Center is a nonpartisan fact tank that informs the public about the issues, attitudes and trends shaping the world. It conducts public opinion polling, demographic research, media content analysis and other empirical social science research. Pew Research Center does not take policy positions. It is a subsidiary of The Pew Charitable Trusts .
How to Write About Coronavirus in a College Essay
Students can share how they navigated life during the coronavirus pandemic in a full-length essay or an optional supplement.
Writing About COVID-19 in College Essays

Getty Images
Experts say students should be honest and not limit themselves to merely their experiences with the pandemic.
The global impact of COVID-19, the disease caused by the novel coronavirus, means colleges and prospective students alike are in for an admissions cycle like no other. Both face unprecedented challenges and questions as they grapple with their respective futures amid the ongoing fallout of the pandemic.
Colleges must examine applicants without the aid of standardized test scores for many – a factor that prompted many schools to go test-optional for now . Even grades, a significant component of a college application, may be hard to interpret with some high schools adopting pass-fail classes last spring due to the pandemic. Major college admissions factors are suddenly skewed.
"I can't help but think other (admissions) factors are going to matter more," says Ethan Sawyer, founder of the College Essay Guy, a website that offers free and paid essay-writing resources.
College essays and letters of recommendation , Sawyer says, are likely to carry more weight than ever in this admissions cycle. And many essays will likely focus on how the pandemic shaped students' lives throughout an often tumultuous 2020.
But before writing a college essay focused on the coronavirus, students should explore whether it's the best topic for them.
Writing About COVID-19 for a College Application
Much of daily life has been colored by the coronavirus. Virtual learning is the norm at many colleges and high schools, many extracurriculars have vanished and social lives have stalled for students complying with measures to stop the spread of COVID-19.
"For some young people, the pandemic took away what they envisioned as their senior year," says Robert Alexander, dean of admissions, financial aid and enrollment management at the University of Rochester in New York. "Maybe that's a spot on a varsity athletic team or the lead role in the fall play. And it's OK for them to mourn what should have been and what they feel like they lost, but more important is how are they making the most of the opportunities they do have?"
That question, Alexander says, is what colleges want answered if students choose to address COVID-19 in their college essay.
But the question of whether a student should write about the coronavirus is tricky. The answer depends largely on the student.
"In general, I don't think students should write about COVID-19 in their main personal statement for their application," Robin Miller, master college admissions counselor at IvyWise, a college counseling company, wrote in an email.
"Certainly, there may be exceptions to this based on a student's individual experience, but since the personal essay is the main place in the application where the student can really allow their voice to be heard and share insight into who they are as an individual, there are likely many other topics they can choose to write about that are more distinctive and unique than COVID-19," Miller says.
Opinions among admissions experts vary on whether to write about the likely popular topic of the pandemic.
"If your essay communicates something positive, unique, and compelling about you in an interesting and eloquent way, go for it," Carolyn Pippen, principal college admissions counselor at IvyWise, wrote in an email. She adds that students shouldn't be dissuaded from writing about a topic merely because it's common, noting that "topics are bound to repeat, no matter how hard we try to avoid it."
Above all, she urges honesty.
"If your experience within the context of the pandemic has been truly unique, then write about that experience, and the standing out will take care of itself," Pippen says. "If your experience has been generally the same as most other students in your context, then trying to find a unique angle can easily cross the line into exploiting a tragedy, or at least appearing as though you have."
But focusing entirely on the pandemic can limit a student to a single story and narrow who they are in an application, Sawyer says. "There are so many wonderful possibilities for what you can say about yourself outside of your experience within the pandemic."
He notes that passions, strengths, career interests and personal identity are among the multitude of essay topic options available to applicants and encourages them to probe their values to help determine the topic that matters most to them – and write about it.
That doesn't mean the pandemic experience has to be ignored if applicants feel the need to write about it.
Writing About Coronavirus in Main and Supplemental Essays
Students can choose to write a full-length college essay on the coronavirus or summarize their experience in a shorter form.
To help students explain how the pandemic affected them, The Common App has added an optional section to address this topic. Applicants have 250 words to describe their pandemic experience and the personal and academic impact of COVID-19.
"That's not a trick question, and there's no right or wrong answer," Alexander says. Colleges want to know, he adds, how students navigated the pandemic, how they prioritized their time, what responsibilities they took on and what they learned along the way.
If students can distill all of the above information into 250 words, there's likely no need to write about it in a full-length college essay, experts say. And applicants whose lives were not heavily altered by the pandemic may even choose to skip the optional COVID-19 question.
"This space is best used to discuss hardship and/or significant challenges that the student and/or the student's family experienced as a result of COVID-19 and how they have responded to those difficulties," Miller notes. Using the section to acknowledge a lack of impact, she adds, "could be perceived as trite and lacking insight, despite the good intentions of the applicant."
To guard against this lack of awareness, Sawyer encourages students to tap someone they trust to review their writing , whether it's the 250-word Common App response or the full-length essay.
Experts tend to agree that the short-form approach to this as an essay topic works better, but there are exceptions. And if a student does have a coronavirus story that he or she feels must be told, Alexander encourages the writer to be authentic in the essay.
"My advice for an essay about COVID-19 is the same as my advice about an essay for any topic – and that is, don't write what you think we want to read or hear," Alexander says. "Write what really changed you and that story that now is yours and yours alone to tell."
Sawyer urges students to ask themselves, "What's the sentence that only I can write?" He also encourages students to remember that the pandemic is only a chapter of their lives and not the whole book.
Miller, who cautions against writing a full-length essay on the coronavirus, says that if students choose to do so they should have a conversation with their high school counselor about whether that's the right move. And if students choose to proceed with COVID-19 as a topic, she says they need to be clear, detailed and insightful about what they learned and how they adapted along the way.
"Approaching the essay in this manner will provide important balance while demonstrating personal growth and vulnerability," Miller says.
Pippen encourages students to remember that they are in an unprecedented time for college admissions.
"It is important to keep in mind with all of these (admission) factors that no colleges have ever had to consider them this way in the selection process, if at all," Pippen says. "They have had very little time to calibrate their evaluations of different application components within their offices, let alone across institutions. This means that colleges will all be handling the admissions process a little bit differently, and their approaches may even evolve over the course of the admissions cycle."
Searching for a college? Get our complete rankings of Best Colleges.
10 Ways to Discover College Essay Ideas

Tags: students , colleges , college admissions , college applications , college search , Coronavirus
2024 Best Colleges
Search for your perfect fit with the U.S. News rankings of colleges and universities.
College Admissions: Get a Step Ahead!
Sign up to receive the latest updates from U.S. News & World Report and our trusted partners and sponsors. By clicking submit, you are agreeing to our Terms and Conditions & Privacy Policy .
Ask an Alum: Making the Most Out of College
You May Also Like
Ways to maximize campus life.
Anayat Durrani March 14, 2024

8 People to Meet on Your College Campus
Sarah Wood March 12, 2024

Completing College Applications on Time
Cole Claybourn March 12, 2024

Colleges Must Foster Civil Debate
Jonathan Koppell March 12, 2024

The Complete Guide to the TOEFL
Sarah Wood March 8, 2024

Unique College Campus Visits
Sarah Wood March 7, 2024

MBA Programs Fail to Attract Women
Joy Jones March 7, 2024

12 Colleges With the Most NBA Players
Cole Claybourn March 1, 2024

Higher Education on the Edge
Alan Mallach Feb. 29, 2024

Disability Accommodations in College
Anayat Durrani Feb. 23, 2024


The Student Voice of Austin Community College District

COVID-19: How a Pandemic Changed The Way We Live
Whether a student or a professor, or working at an office, or at a store, life has changed. As the number of cases in Travis and Williamson County continues to rise, life will continue to be different and will never be the same.

By: Angela Murillo Martinez
It is no surprise that nobody’s life is the same as it was before the pandemic occurred. Whether a student or a professor, or working at an office, or at a store, life has changed. As the number of cases in Travis and Williamson County continues to rise, life will continue to be different and will never be the same. Many have had to embrace change as they’ve had to continue working or even going to school, and as time continues it becomes more of a new reality. New routines are being built and embraced openly as there is no other option, but to continue in the midst of a pandemic.
According to the CDC, as of July 25th, the total number of cases in the whole United States is 4,099,310. A major spike in cases occurred as many states allowed public spaces to re-open such as stores, amusement parks, churches, workplaces, and many more. In the state of Texas, it is reported that there are 369,826 cases. Although the number of cases continues to rise in the state, public spaces in the state continue to remain open. In Williamson County alone, so far 5,145 cases have been reported in one day, and in Travis County, 18,939 cases have been reported.
It is important to remember to follow safety procedures to avoid furthering the spread of COVID-19 and to make sure that everyone remains healthy and safe. If one finds themselves going out, don’t forget to bring a face covering. As of the third of July, all Texans are required to wear face masks in public spaces. Failure to comply with such orders may result in a warning at first and in further violations, one can be fined up to $250. Additionally, it is important to respect the space of others and maintain a six feet distance when out in public. The Texas Health and Human Services also recommends washing one’s hands often with soap and water for 20 seconds and also mentions avoiding touching one’s face with unwashed hands. Amongst other actions shared on their website to prevent the spread of COVID-19, an important one is too often disinfected surfaces that are often touched by others.
With this being said, people have to keep working, students have to continue going to school, and in general, life has to continue. The only difference now is exactly how life is being continued by people. For Stephanie Murillo, a student studying criminal justice and obtaining her paralegal certification, she has had to not only adjust to a new job but also adjust to working from home and taking online classes. It had been only two weeks at her new job as a court clerk when her office was closed and she had to start working remotely. Now it’s been five months and she’s had to learn everything through zoom calls and emails, while also managing her online classes. She admits that it has been hard having to manage to work at home and taking online classes, especially since her hours at work have extended. No longer being able to follow the usual seven to five schedule she had been following before the pandemic. “Before I was able to leave work at five and it would stay there, and I would be able to come home or go to school.
But now I just feel like I work extra hours because my office is my room.” On top of that, she admits that taking her classes online has required more time and commitment. To her, it seems that her days have only gotten longer and the workload has become heavier.
Furthermore, she has felt it was a difficult transition to have to learn everything she needed to know remotely and to also learn how to manage all the technology necessary to continue. “I was in the process of learning my new position but then when the pandemic started, I had to be trained in something that was new to my co-workers, which was working remotely from home.” Despite the difficulties and challenges she has had to face, she has grown to like working from home and admits that she will find it difficult to return to the office. Although she’s been told that they will return to the office since June, so far the official date is still uncertain and continues to change as the situation escalates. They have planned to return to the office on August 17th, though this isn’t a set date. So for now, she continues to work remotely and learn as much as she can while being physically apart from her co-workers.
For other students such as Kylie Birchfield, a talented photographer studying photography, she’s had more time to focus on her passion. Though she did find the last couple of months left in the Spring semester difficult as a result of transitioning to online classes, she has found herself with more free time on her hands as a result of the pandemic. Not only has she been able to work more on her own personal photography projects, but she’s also been able to get an internship with Austin Woman Magazine . “I know not a lot of people have gotten good things out of this, but for me, I’ve had a lot of good things come out of it.” In her internship with the magazine, she has been able to do a feature with them on COVID-19 where she photographed three women who find themselves on the front lines of the fight against the pandemic.
She has found that as more people spend more time on social media, the more people she has finding her page and lining up to work with her. Although now, there are certain safety procedures she follows to avoid furthering the spread of COVID-19 such as maintaining a distance and wearing a mask when working with others. As the previously mentioned guidelines are more implement into one’s new daily routine, she often has to remind herself of bringing her masks and maintaining a distance at photoshoots.
“Sometimes I have to rethink what I’m doing in photoshoots. I can’t get up close, can’t move their hair, I have to ask them to move their hair around.”
With this being said, she continues to find herself with more opportunities and considers this a “kickstart” for her career. Despite losing her job as a result of the pandemic, she finds herself blessed to have the free time she has now and has been using it to do what she loves.
Others like Mary Monk, a student studying Government, no longer finds herself having to commute to her classes. Hence, saving her time that she would spend taking the bus and traveling from class to class. While she did find it hard to transition to online classes at the end of the Spring semester, she realized that in most of her classes they were easy to finish without meeting in person. As a result of the pandemic, she has found it hard to find an internship or a
“Your Freshman summer is supposed to be the time where you get internships and jobs, and it’s so hard because I applied to so many internships and they’ve just been like ‘oh, we have to see because of COVID’… So it’s been really difficult in that regard,” said Monk
Although Monk was used to her friends going to different schools and living far, resulting in not being able to see each other often. She now finds herself talking more consistently with them through text and video calls.
“With family, at first, I think we were all on the same page, but as time goes on, and people are in their homes for longer, our family gets a little divisive on what we should be doing, and what caution we should be taking,” said Monk
But as far as her immediate family, she finds herself at home with them safely and spending more time together as they are unable to go out. As she continues to take online classes, she sees this as an opportunity to further her studies.
“I feel like I can take on more than I probably thought I could if I had to do them all in person because with actually going to school, physically, you have to take into account how long it’s going to take you to go from one building to another.”
Now, Monk takes her classes online, her room becomes her classroom and she no longer has to leave it to attend class. She plans that if the pandemic continues on for longer, which she thinks it will, she will most definitely take more classes and hopes to find an internship that can begin to prepare her for her career.
Despite being unable to meet on campus or be physical together, organizations are still continuing to meet through video calls. One of those organizations being the German club, which has met every three weeks during the summer. Although there are certain things that have changed and other things that they are no longer able to do since moving to video calls, the club hasn’t changed that much. “We do the same things, we just do them differently. We used to play board games, and we obviously don’t do that anymore, but we played hangman at a bunch of the meetings I remember going to, and we still play hangman online,” said the club president Lauren Sanders.
Though their group has gotten smaller since they transitioned to video calls, they have built a small, defined group who all meet together and converse in both German and English. They do admit that it has been harder to get people involved since they are no longer able to put posters around the Highland campus or have people show up after German class, but still, they continue to meet and encourage that all those interested in German no matter the level of expertise, to join them.
Since the pandemic started, the club never planned on stopping and quickly continued moving forward.
“I thought the club was going to end, seeing how things were going, only a few of us were left. But when they were saying, we have to decide who’s going to be the president, treasurer, and secretary, ‘I was like ok, we’re still doing this. I’m in’ and I mean it’s something to do when I’m at the house quarantining all day,” said Emiliano Antunano.
This same resilience has kept them going through the pandemic and continues to push them despite having to continue meeting online in the upcoming fall semester. The club which consists of German speakers of all levels has a supportive and welcoming community, where they are all helping each other improve their German, but also keep each other company in the midst of the pandemic. In the words of a club
member,
“I hope to go to the in-person meeting when all this ends since I haven’t been able to go to those since I joined after all this happened,” said Marshall Brown.
While life had seemed to pause at the beginning of the pandemic, people were unable to continue like this forever, and life has had to continue. As people begin to return to work at their offices or at stores or begin to go out again or return to campus, it doesn’t mean that the pandemic has completely gone away. If anything, the number of cases continues to rise, and therefore, everyone should continue to be careful to protect not only their health but the health of others. Everyone is having to face a new reality and is experiencing new routines, so no one is alone in this situation. Although life continues with uncertainty, if everyone works together and follows the necessary precautions, soon we’ll be able to all be together again on campus.
For this and more stories like this
College essay samples
How 2020 and covid-19 changed my life.
Usually people like the New Year not only because they expect something unusual and great to happen during holidays, but also they hope that the coming year is going to bring a lot of positive changes to their lives and that they will gain new opportunities for self- realization, will have new contacts and friends and so on.
When the year 2020 started, I could not even imagine what kind of significant changes it was going to bring into my life as well as to the lives of millions of people worldwide. I think nobody could expect that we will have to face an absolutely different reality and cope with absolutely different problems, which we were used to in our normal lives. I am convinced that the year 2020 has impacted each single individual on our planet to some extent.
I heard a lot about thinking positively before, but I have always associated it with some minor everyday things, like for example conflicting with your parents. You should not feel desperate, just relax and do your best to solve the problem and leave the conflict in the past. Or when you have a difficult exam for example, you should not be tense and stressed, this will not help you to do your best during it or you might even fail. Instead, it is better to think positively and try your hardest.
The year 2020 has shown to me that the real meaning of thinking positively is much deeper and more serious in comparison to everyday problems. I have found out that there are much more problems in our lives, than I could imagine before. First of all you should constantly feel under the pressure of the risks, related to the virus. Everybody has ageing family members and realization of the fact of their current vulnerability makes you change your attitude to them and to communication with them in a different way.
Actually, any close person is at risk, thus you constantly feel that you want to protect your family, your close people from getting sick and risking their lives. I have some of my friends, who started to have psychological problems, because of the isolation and COVID -19 dangers. I did my best to support them and here I remembered again about the real meaning of thinking positively. You should think positively for the sake of other people, who turn out to be not that strong as you, either physically or mentally.
The year 2020 has revealed to me other life truths as well. For example I have learnt to appreciate the things, which I used to accept as ordinary ones before. I appreciate the opportunity to spend time with my beloved people, I appreciate the time spent outside, in the park for example, I started to like any kind of weather, as it is not that important, whether it is raining, or it is hot, you can always find the ways to comfort yourself if you continue to think positively.
I learnt how to notice some nice things and to focus upon them, instead of thinking about dangers, related to coronavirus and plunging into depression. I have experienced the pleasure of physical exercise without any specially organized conditions, just at home or in the park near my home. From now on my regular sport activities contribute to my way of positive thinking. I continue to exercise my positive thinking and to add new notes and aspects to it. I become more open towards new experiences and ideas in my life and this is the most important change, which happened to me in 2020.
Do you like this essay?
Our writers can write a paper like this for you!
Order your paper here .
- High contrast
- About UNICEF
- Where we work
- Explore careers
- Working in emergencies
- Diversity and inclusion
- Leadership recruitment
- Support UNICEF
- Search jobs
- Candidate login
Search UNICEF
"my view of life changed when i got covid-19", agnes barongo, communication for development specialist in uganda, realized firsthand the impact of covid-19 on women's lives.
On March 8 , it's International Women's Day . This year’s theme is " Women in leadership: Achieving an equal future in a COVID-19 world ", celebrating the tremendous efforts by women around the world in shaping a more equal future and recovery from the COVID-19 pandemic. At UNICEF , we want to celebrate the achievements of women in leadership positions, and also those who display leadership qualities.
Throughout the whole month of March 2021, the Women's Month , we publish the stories of only a few of the many women who make a difference in UNICEF every day. Today, we host the interview of Agnes Barongo , our Communications for Development (C4D) Specialist in UNICEF U ganda

My life view changed just before Christmas when I got COVID-19. I was utterly shocked and kept asking how I could fail at observing the prevention protocols. Now I truly understand the psychological and physical meaning of living with COVID19. Not everyone is fortunate to have ready access to social services, so I am fortunate. But the experience provided me with further compassion and determination to keep doing the best to ensure less fortunate citizens get access to the right information and services that can save their lives
Agnes Barongo
Communications for Development (C4D) Specialist, Uganda
Who are you and what is your role at UNICEF?
I hail from Hoima District, located in mid-western Uganda. It is one of 135 districts in the Republic of Uganda that has a total population of 45.7 million people. Its capital, Hoima City, has just been converted into a city as part of the development agenda to upgrade Municipal Town Councils around the nation. I work as a Communication for Development Specialist based in Kampala City, the capital of the Republic of Uganda. My main responsibilities centre on ensuring that bottlenecks to the adoption of positive behaviourial and societal practices are addressed at different levels in our society from the household, to the community, to the district and national levels. I work with the Education and Child Protection teams in UNICEF, Government and Civil Society Organizations to have these addressed in the first and second decades of a child’s life. Presently, I work in 30 focus districts and with eight government line ministries to ensure that both at the community and national levels, there are systems running in place to support vulnerable children to have access to education and child protection social services.
How did COVID-19 impact your life, both on professional as well as on personal level?
On a professional level COVID-19 provided me with a revisit to emergency work that I had already been supporting as the alternative focal point in the Communication for Development Unit, under the Communications and Partnerships Section in UNICEF Uganda Country Office. I had already been part of the emergency interventions supporting the Ministry of Health under the Public Health Emergency Operations Centre and National Task Force during the 2017 Marburg outbreak in Eastern Uganda and the 2018 – 2019 Ebola Virus Disease outbreak in Western Uganda. Health emergencies being a cross-sectoral programme I had already experienced what it means to ensure that the all the education and child protection stakeholders convene to discuss and take action on addressing the virulent outbreaks. I also was able to understand in these two outbreaks the vital importance of being vigilant and being the example to demonstrating how to stick to Standard Operating Procedures (SOPs) when it came to personal and team safety measures. When COVID-19 broke out, I was on leave, however, my prior experience with emergencies and virulent outbreaks made me more conscious and empathetic to the communities around me. Not everyone responds to directives set out by government or district officials. My job continues to provide me with perspectives on how there needs to be a re-invention each time to see how best to encourage people to keep adhering to positive social and behaviourial practices that would keep them safe from obtaining any deadly virus of epidemic proportions, infecting people and dying a death that could be prevented. I found myself greeting strangers, advising them on the protocols for protecting themselves from COVID-19. I also did get into situations where I would inquire from a service delivery point why there was no sanitizer, washing point or temperature gun present. Of course, in these circumstances, it was imperative to have a demonstrative level of understanding, humility but at the same time determination in getting the safety protocols message across to the people in the communities I interacted in. At a personal level, the COVID-19 situation made me learn to understand my family better. During lockdown, there were various moments of epiphany, living in a household with extended family members. Inadvertently, the proximity helped me to understand and become more empathetic to the individual challenges we as humans face daily. I am less judgmental now when it comes to reviewing cases of violence because I realized that our upbringing colluding with our immediate environment and personal difficulties in attaining a sustainable living, can bring out the worst behaviourial traits. I try not to make excuses but at least I have a more varied approach to making inquiries into trying to understand what drives each human being to perform an act of violence against family or strangers.
My life view changed just before Christmas when I got COVID-19. I was utterly shocked and kept asking how I could fail at observing the prevention protocols. However, it also made me ensure that I paid acute attention to treatment. I reported daily to the UN doctor in charge and took medication and monitored my vitals. When I went for the exit COVID-19 test, I was extremely nervous and did not sleep the night before. The following day when I got my results, there was an explosion of relief. Now I truly understand the psychological and physical meaning of living with COVID19. I am a better person when it comes to vigilance in observing prevention protocols and to the occasional dismay of my family, I keep repeating the SOPs because I understand firsthand how the pandemic has impacted on me.

Not everyone is fortunate to have readily access to social services, so I am fortunate. But it provides me with further compassion and determination to keep doing the best to ensure less fortunate citizens get access to the right information and services that can save their lives.
Do you think that the COVID-19 pandemic disproportionally impacted women, mothers and girls' lives, and how?
To a great extent everyone was impacted negatively by this COVID-19 pandemic. Until adequate research is done on a nationwide survey in Uganda, it would be presumptuous to say that women, mothers and girls lives were disproportionally impacted without actual statistics per household, village, parish, sub-county and district. But based on Uganda Broadcast and Print Media articles, Child Helpline reports and research with a focus on two publications. The Violence Against Children Survey - Ministry of Gender, Labour and Social Development 2018 and the Adolescent Vulnerability Index - Government of Uganda and Population Council 2013, yes women, mothers and girls have suffered the brunt of the COVID-19 pandemic. Girls have dropped out of school now that education was haltered for 12 months since March last year. If a girl child is in a household where the decision maker, felt there was need for her to get married based on her biological maturity, then she was unlawfully sent to cohabit with a man. In return, gifts in form of bride price exchange hands and this union is based on transactional parameters. A number of Mothers spoken to have occasionally stated that their daughters would receive health and protection from the man they have been forced into a union with. For these particular women, their mindset makes them believe that a traditional union with a man is the solution to security and protection. These women unfortunately do not see value in the girl child staying at home, working with her parents to continue learning as a way of protecting her from any harmful traditional practice of child marriage, teenage pregnancy while waiting for schools to reopen. In this dichotomy of the girl child facing violence and their Mothers, Aunties, Grandmothers witnessing this rights abuse, are their voices not being heard or respected by the decision maker in the household who is the perpetuator. There have been reports of an escalation of violence at homes, domestic, sexual and psychological. As candidate and sub-candidate classes have recently resumed schooling, School teachers have already obtained reports from students who are suffering from the aftermath of these various forms of violence they experienced or witness as it was unleashed on the female adults in their families and communities. A recommendation made by the Gender Unit, Ministry of Education and Sports stipulates there is an urgent requirement for psyscho-social support to be provided to students on return to school. In our nation where social services in the field of pyscho-social support is still gaining traction, more would need to be done to strengthen the systems that can provide this to Women, Mothers, Aunties and Grandmothers.
What do you believe are women's strengths, and what are the advantages of female leadership in combatting the COVID-19 pandemic?
The age-old adage is when you educate a girl, you educate a nation is true. Government strategies that focus attention on the girls providing them with opportunities at primary, secondary, tertiary and university levels have clearly demonstrated a rise in young women striving ahead to be leaders in different sectors in the nation. Women are naturals when it comes to nurturing people in their spheres of influence. This has been seen on a regular basis when it comes to the health system at community level. Village Health Teams - are leaders in their own right. They constitute of women that conduct more household visits and are easily better welcomed by families and listened too in the adoption of social and behaviourial practices. Furthermore, when female district officials address communities during rallies or through community radios on the benefits of adoption of positive social and behaviourial practices that focus on education, protection and health, there is usually better reception. This has been seen the uptake of Reproductive, Maternal, Neo-natal, Child, Adolescent Health services at health facilities and Enrollment of girl-child in schools over the last 20 years nationwide. At the national level, in the context of COVID-19, women leaders have further demonstrated that they can make the positive difference in curbing the rapid spread of the pandemic. The two top health officials in the Republic of Uganda are women, the Minister of Health - Dr. Jane Acheng, the Minister of State for Health (Primary Health Care) Dr. Moriku Joyce Kaducu and the Permanent Secretary - Dr. Diana Atwine gain attention during their weekly addresses to the public. They have a special measure of appeal to communities as they provide simple actions that each family unit, organization and district can adopt to ensure they benefit from not getting the COVID-19 virus. They also further illustrate that adoption of Standard Operating Procedures (SOPs) has health and economic benefits which is vital in the field of social and behavior change if you want communities to work towards prevention and response in addressing the spread of COVID-19.
What is your advice to women navigating their careers during a health crisis, as well as in a post COVID-19 pandemic world?
Persistence should always prevail. Women should keep focused on doing their best even with the hardship of family responsibilities in the unique environment of closed schools, curfews and partial lockdowns. They should never give up on their dreams to excel and take up opportunities that would provide them with more scope to experience and provide results in the development agenda of their communities and nation. On one level, COVID-19 has demonstrated to women, that they can be caretakers of families at the same be professionals at the workplace to ensure they play a nationalist role, doing their duty and saving lives. At another level, women who have had to stay away from their loved ones in other countries owing to nation lockdowns for a year are further demonstrating as that they are there to offer services in the countries they are working in, sacrificing time otherwise spent with their loved ones because they believe that humanity needs their call to duty. It is an extreme period but post COVID-19, I believe the aftereffects would make our human selves more empathetic because COVID-19 has demonstrated that when everyone works together, they can defeat a common enemy to Life, Development and Prosperity.
Related topics
More to explore, unicef women leading the fight for children.
On the International Women's Day 2021, we celebrate the stories of strong UNICEF women in leadership positions
"Look for the opportunity in every situation and grab it!"
Anna Mensah, Senior Executive Associate in Ghana, saw opportunities and challenges in the pandemic
Investing in a workplace where women can thrive
Our workplace reflects the world we want to live in: gender-equal, with opportunity and empowerment for all.
Opportunities for German nationals through the JPO programme
Young professionals who are nationals of Germany can apply to join UNICEF as Junior Professional Officers
/media/video/upload/Opener_rt.mp4)
How Science Beat the Virus
And what it lost in the process

Listen to this article
Listen to more stories on audm
This article was published online on December 14, 2020.
In fall of 2019, exactly zero scientists were studying COVID‑19, because no one knew the disease existed. The coronavirus that causes it, SARS‑CoV‑2, had only recently jumped into humans and had been neither identified nor named. But by the end of March 2020, it had spread to more than 170 countries, sickened more than 750,000 people, and triggered the biggest pivot in the history of modern science. Thousands of researchers dropped whatever intellectual puzzles had previously consumed their curiosity and began working on the pandemic instead. In mere months, science became thoroughly COVID-ized.
As of this writing, the biomedical library PubMed lists more than 74,000 COVID-related scientific papers—more than twice as many as there are about polio, measles, cholera, dengue, or other diseases that have plagued humanity for centuries. Only 9,700 Ebola-related papers have been published since its discovery in 1976; last year, at least one journal received more COVID‑19 papers than that for consideration. By September, the prestigious New England Journal of Medicine had received 30,000 submissions—16,000 more than in all of 2019. “All that difference is COVID‑19,” Eric Rubin, NEJM ’s editor in chief, says. Francis Collins, the director of the National Institutes of Health, told me, “The way this has resulted in a shift in scientific priorities has been unprecedented.”
Much like famous initiatives such as the Manhattan Project and the Apollo program, epidemics focus the energies of large groups of scientists. In the U.S., the influenza pandemic of 1918, the threat of malaria in the tropical battlegrounds of World War II, and the rise of polio in the postwar years all triggered large pivots. Recent epidemics of Ebola and Zika each prompted a temporary burst of funding and publications . But “nothing in history was even close to the level of pivoting that’s happening right now,” Madhukar Pai of McGill University told me.
That’s partly because there are just more scientists: From 1960 to 2010, the number of biological or medical researchers in the U.S. increased sevenfold , from just 30,000 to more than 220,000. But SARS-CoV-2 has also spread farther and faster than any new virus in a century. For Western scientists, it wasn’t a faraway threat like Ebola. It threatened to inflame their lungs. It shut down their labs. “It hit us at home,” Pai said.
In a survey of 2,500 researchers in the U.S., Canada, and Europe, Kyle Myers from Harvard and his team found that 32 percent had shifted their focus toward the pandemic. Neuroscientists who study the sense of smell started investigating why COVID‑19 patients tend to lose theirs. Physicists who had previously experienced infectious diseases only by contracting them found themselves creating models to inform policy makers. Michael D. L. Johnson at the University of Arizona normally studies copper’s toxic effects on bacteria. But when he learned that SARS‑CoV‑2 persists for less time on copper surfaces than on other materials, he partially pivoted to see how the virus might be vulnerable to the metal. No other disease has been scrutinized so intensely, by so much combined intellect, in so brief a time.
These efforts have already paid off. New diagnostic tests can detect the virus within minutes. Massive open data sets of viral genomes and COVID‑19 cases have produced the most detailed picture yet of a new disease’s evolution. Vaccines are being developed with record-breaking speed. SARS‑CoV‑2 will be one of the most thoroughly characterized of all pathogens, and the secrets it yields will deepen our understanding of other viruses, leaving the world better prepared to face the next pandemic.
But the COVID‑19 pivot has also revealed the all-too-human frailties of the scientific enterprise . Flawed research made the pandemic more confusing, influencing misguided policies. Clinicians wasted millions of dollars on trials that were so sloppy as to be pointless. Overconfident poseurs published misleading work on topics in which they had no expertise. Racial and gender inequalities in the scientific field widened.
Amid a long winter of sickness , it’s hard not to focus on the political failures that led us to a third surge. But when people look back on this period, decades from now, they will also tell stories, both good and bad, about this extraordinary moment for science. At its best, science is a self-correcting march toward greater knowledge for the betterment of humanity. At its worst, it is a self-interested pursuit of greater prestige at the cost of truth and rigor. The pandemic brought both aspects to the fore. Humanity will benefit from the products of the COVID‑19 pivot. Science itself will too, if it learns from the experience.
In February, Jennifer Doudna, one of America’s most prominent scientists, was still focused on CRISPR—the gene-editing tool that she’d co-discovered and that won her a Nobel Prize in October. But when her son’s high school shut down and UC Berkeley, her university, closed its campus, the severity of the impending pandemic became clear. “In three weeks, I went from thinking we’re still okay to thinking that my whole life is going to change,” she told me. On March 13, she and dozens of colleagues at the Innovative Genomics Institute, which she leads, agreed to pause most of their ongoing projects and redirect their skills to addressing COVID‑19. They worked on CRISPR-based diagnostic tests. Because existing tests were in short supply, they converted lab space into a pop-up testing facility to serve the local community. “We need to make our expertise relevant to whatever is happening right now,” she said.
Scientists who’d already been studying other emerging diseases were even quicker off the mark. Lauren Gardner, an engineering professor at Johns Hopkins University who has studied dengue and Zika, knew that new epidemics are accompanied by a dearth of real-time data. So she and one of her students created an online global dashboard to map and tally all publicly reported COVID‑19 cases and deaths. After one night of work, they released it, on January 22. The dashboard has since been accessed daily by governments, public-health agencies, news organizations, and anxious citizens.
Studying deadly viruses is challenging at the best of times, and was especially so this past year. To handle SARS‑CoV‑2, scientists must work in “biosafety level 3” labs, fitted with special airflow systems and other extreme measures; although the actual number is not known, an estimated 200 such facilities exist in the U.S. Researchers often test new drugs and vaccines on monkeys before proceeding to human trials, but the U.S. is facing a monkey shortage after China stopped exporting the animals, possibly because it needed them for research. And other biomedical research is now more difficult because of physical-distancing requirements. “Usually we had people packed in, but with COVID, we do shift work,” Akiko Iwasaki, a Yale immunologist, told me. “People are coming in at ridiculous hours” to protect themselves from the very virus they are trying to study.
Recommended Reading

What the Chaos in Hospitals Is Doing to Doctors

How the Pandemic Defeated America

Candy Land Was Invented for Polio Wards
Experts on emerging diseases are scarce: These threats go neglected by the public in the lulls between epidemics. “Just a year ago I had to explain to people why I was studying coronaviruses,” says Lisa Gralinski of the University of North Carolina at Chapel Hill. “That’s never going to be a concern again.” Stressed and stretched, she and other emerging-disease researchers were also conscripted into unfamiliar roles. They’re acting as makeshift advisers to businesses, schools, and local governments. They’re barraged by interview requests from journalists. They’re explaining the nuances of the pandemic on Twitter, to huge new follower counts. “It’s often the same person who’s helping the Namibian government to manage malaria outbreaks and is now being pulled into helping Maryland manage COVID‑19,” Gardner told me.
But the newfound global interest in viruses also means “you have a lot more people you can talk through problems with,” Pardis Sabeti, a computational geneticist at the Broad Institute of MIT and Harvard, told me. Indeed, COVID‑19 papers are more likely than typical biomedical studies to have authors who had never published together before, according to a team led by Ying Ding, who works at the University of Texas at Austin.
Fast-forming alliances could work at breakneck speed because many researchers had spent the past few decades transforming science from a plodding, cloistered endeavor into something nimbler and more transparent. Traditionally, a scientist submits her paper to a journal, which sends it to a (surprisingly small) group of peers for (several rounds of usually anonymous) comments; if the paper passes this (typically months-long) peer-review gantlet, it is published (often behind an expensive paywall). Languid and opaque, this system is ill-suited to a fast-moving outbreak. But biomedical scientists can now upload preliminary versions of their papers, or “preprints,” to freely accessible websites, allowing others to immediately dissect and build upon their results. This practice had been slowly gaining popularity before 2020, but proved so vital for sharing information about COVID‑19 that it will likely become a mainstay of modern biomedical research. Preprints accelerate science, and the pandemic accelerated the use of preprints. At the start of the year, one repository, medRxiv (pronounced “med archive”), held about 1,000 preprints. By the end of October, it had more than 12,000.
Open data sets and sophisticated new tools to manipulate them have likewise made today’s researchers more flexible. SARS‑CoV‑2’s genome was decoded and shared by Chinese scientists just 10 days after the first cases were reported. By November, more than 197,000 SARS‑CoV‑2 genomes had been sequenced. About 90 years ago, no one had even seen an individual virus; today, scientists have reconstructed the shape of SARS‑CoV‑2 down to the position of individual atoms. Researchers have begun to uncover how SARS‑CoV‑2 compares with other coronaviruses in wild bats, the likely reservoir; how it infiltrates and co-opts our cells; how the immune system overreacts to it, creating the symptoms of COVID‑19. “We’re learning about this virus faster than we’ve ever learned about any virus in history,” Sabeti said.
By March, the odds of quickly eradicating the new coronavirus looked slim. A vaccine became the likeliest endgame, and the race to create one was a resounding success. The process normally takes years, but as I write this, 54 different vaccines are being tested for safety and efficacy, and 12 have entered Phase 3 clinical trials—the final checkpoint. As of this writing, Pfizer/BioNTech and Moderna have announced that, based on preliminary results from these trials, their respective vaccines are roughly 95 percent effective at preventing COVID‑19. * “We went from a virus whose sequence was only known in January, and now in the fall, we’re finishing— finishing —a Phase 3 trial,” Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases and a member of the White House’s coronavirus task force, told me. “Holy mackerel.”
Most vaccines comprise dead, weakened, or fragmented pathogens, and must be made from scratch whenever a new threat emerges. But over the past decade, the U.S. and other countries have moved away from this slow “one bug, one drug” approach. Instead, they’ve invested in so-called platform technologies, in which a standard chassis can be easily customized with different payloads that target new viruses. For example, the Pfizer/BioNTech and Moderna vaccines both consist of nanoparticles that contain pieces of SARS‑CoV‑2’s genetic material—its mRNA. When volunteers are injected with these particles, their cells use the mRNA to reconstruct a noninfectious fragment of the virus, allowing their immune system to prepare antibodies that neutralize it. No company has ever brought an mRNA vaccine to market before, but because the basic platform had already been refined, researchers could quickly repurpose it with SARS‑CoV‑2’s mRNA. Moderna got its vaccine into Phase 1 clinical trials on March 16, just 66 days after the new virus’s genome was first uploaded—far faster than any pre-COVID vaccine.
Meanwhile, companies compressed the process of vaccine development by running what would normally be sequential steps in parallel, while still checking for safety and efficacy. The federal government’s Operation Warp Speed, an effort to accelerate vaccine distribution, funded several companies at once—an unusual move. It preordered doses and invested in manufacturing facilities before trials were complete, reducing the risk for pharmaceutical companies looking to participate. Ironically, federal ineptitude at containing SARS‑CoV‑2 helped too. In the U.S., “the fact that the virus is everywhere makes it easier to gauge the performance of a vaccine,” says Natalie Dean of the University of Florida, who studies vaccine trials. “You can’t do a [Phase 3] vaccine trial in South Korea,” because the outbreak there is under control.
Read: How the pandemic will end
Vaccines will not immediately end the pandemic . Millions of doses will have to be manufactured, allocated, and distributed ; large numbers of Americans could refuse the vaccine ; and how long vaccine-induced immunity will last is still unclear. In the rosiest scenario, the Pfizer/BioNTech and Moderna vaccines are approved and smoothly rolled out over the next 12 months. By the end of the year, the U.S. achieves herd immunity, after which the virus struggles to find susceptible hosts. It still circulates, but outbreaks are sporadic and short-lived. Schools and businesses reopen. Families hug tightly and celebrate joyously over Thanksgiving and Christmas.
And the next time a mystery pathogen emerges, scientists hope to quickly slot its genetic material into proven platforms, and move the resulting vaccines through the same speedy pipelines that were developed during this pandemic. “I don’t think the world of vaccine development will ever be the same again,” says Nicole Lurie of the Coalition for Epidemic Preparedness Innovations.

As fast as the vaccine-development process was, it could have been faster. Despite the stakes, some pharmaceutical companies with relevant expertise chose not to enter the race, perhaps dissuaded by intense competition. Instead, from February to May, the sector roughly tripled its efforts to develop drugs to treat COVID‑19, according to Kevin Bryan, an economist at the University of Toronto. The decades-old steroid dexamethasone turned out to reduce death rates among severely ill patients on ventilators by more than 12 percent. Early hints suggest that newer treatments such as the monoclonal-antibody therapy bamlanivimab, which was just approved for emergency use by the FDA, could help newly infected patients who have not yet been hospitalized. But although these wins are significant, they are scarce. Most drugs haven’t been effective. Health-care workers became better at saving hospitalized patients more through improvements in basic medical care than through pharmaceutical panaceas—a predictable outcome, because antiviral drugs tend to offer only modest benefits.
The quest for COVID‑19 treatments was slowed by a torrent of shoddy studies whose results were meaningless at best and misleading at worst. Many of the thousands of clinical trials that were launched were too small to produce statistically solid results. Some lacked a control group—a set of comparable patients who received a placebo, and who provided a baseline against which the effects of a drug could be judged. Other trials needlessly overlapped. At least 227 involved hydroxychloroquine—the antimalarial drug that Donald Trump hyped for months. A few large trials eventually confirmed that hydroxychloroquine does nothing for COVID‑19 patients, but not before hundreds of thousands of people were recruited into pointlessly small studies . More than 100,000 Americans have also received convalescent plasma—another treatment that Trump touted. But because most were not enrolled in rigorous trials, “we still don’t know if it works—and it likely doesn’t,” says Luciana Borio, the former director for medical and biodefense preparedness at the National Security Council. “What a waste of time and resources.”
Read: How we survive the winter
In the heat of a disaster, when emergency rooms are filling and patients are dying, it is hard to set up one careful study, let alone coordinate several across a country. But coordination is not impossible. During World War II , federal agencies unified private companies, universities, the military, and other entities in a carefully orchestrated effort to speed pharmaceutical development from benchtop to battlefield. The results—revolutionary malaria treatments, new ways of mass-producing antibiotics, and at least 10 new or improved vaccines for influenza and other diseases—represented “not a triumph of scientific genius but rather of organizational purpose and efficiency,” Kendall Hoyt of Dartmouth College has written.
Similar triumphs occurred last year—in other countries. In March, taking advantage of the United Kingdom’s nationalized health system, British researchers launched a nationwide study called Recovery, which has since enrolled more than 17,600 COVID‑19 patients across 176 institutions. Recovery offered conclusive answers about dexamethasone and hydroxychloroquine and is set to weigh in on several other treatments. No other study has done more to shape the treatment of COVID‑19. The U.S. is now catching up. In April, the NIH launched a partnership called ACTIV , in which academic and industry scientists prioritized the most promising drugs and coordinated trial plans across the country. Since August, several such trials have started. This model was late, but is likely to outlast the pandemic itself, allowing future researchers to rapidly sort medical wheat from pharmaceutical chaff. “I can’t imagine we’ll go back to doing clinical research in the future the way we did in the past,” the NIH’s Francis Collins said.
Even after the COVID‑19 pandemic, the fruits of the pivot will leave us better equipped for our long and intensifying war against harmful viruses. The last time a virus caused this much devastation—the flu pandemic of 1918—scientists were only just learning about viruses, and spent time looking for a bacterial culprit. This one is different. With so many scientists observing intently as a virus wreaks its horrible work upon millions of bodies, the world is learning lessons that could change the way we think about these pathogens forevermore.
Consider the long-term consequences of viral infections. Years after the original SARS virus hit Hong Kong in 2003, about a quarter of survivors still had myalgic encephalomyelitis—a chronic illness whose symptoms, such as extreme fatigue and brain fogs, can worsen dramatically after mild exertion. ME cases are thought to be linked to viral infections, and clusters sometimes follow big outbreaks. So when SARS‑CoV‑2 started spreading, people with ME were unsurprised to hear that tens of thousands of COVID‑19 “long-haulers” were experiencing incapacitating symptoms that rolled on for months . “Everyone in my community has been thinking about this since the start of the pandemic,” says Jennifer Brea, the executive director of the advocacy group #MEAction.
ME and sister illnesses such as dysautonomia, fibromyalgia, and mast cell activation syndrome have long been neglected, their symptoms dismissed as imaginary or psychiatric. Research is poorly funded, so few scientists study them. Little is known about how to prevent and treat them. This negligence has left COVID‑19 long-haulers with few answers or options, and they initially endured the same dismissal as the larger ME community. But their sheer numbers have forced a degree of recognition. They started researching, cataloging their own symptoms. They gained audiences with the NIH and the World Health Organization. Patients who are themselves experts in infectious disease or public health published their stories in top journals. “Long COVID” is being taken seriously, and Brea hopes it might drag all post-infection illnesses into the spotlight. ME never experienced a pivot. COVID‑19 might inadvertently create one.
Anthony Fauci hopes so. His career was defined by HIV, and in 2019 he said in a paper he co-wrote that “the collateral advantages of” studying HIV “have been profound.” Research into HIV/AIDS revolutionized our understanding of the immune system and how diseases subvert it. It produced techniques for developing antiviral drugs that led to treatments for hepatitis C. Inactivated versions of HIV have been used to treat cancers and genetic disorders. From one disease came a cascade of benefits. COVID‑19 will be no different. Fauci had personally seen cases of prolonged symptoms after other viral infections, but “I didn’t really have a good scientific handle on it,” he told me. Such cases are hard to study, because it’s usually impossible to identify the instigating pathogen. But COVID‑19 has created “the most unusual situation imaginable,” Fauci said—a massive cohort of people with long-haul symptoms that are almost certainly caused by one known virus. “It’s an opportunity we cannot lose,” he said.
Read: The core lesson of the COVID-19 heart debate
COVID‑19 has developed a terrifying mystique because it seems to behave in unusual ways. It causes mild symptoms in some but critical illness in others. It is a respiratory virus and yet seems to attack the heart, brain, kidneys, and other organs. It has reinfected a small number of people who had recently recovered. But many other viruses share similar abilities; they just don’t infect millions of people in a matter of months or grab the attention of the entire scientific community. Thanks to COVID‑19, more researchers are looking for these rarer sides of viral infections, and spotting them.
At least 20 known viruses, including influenza and measles, can trigger myocarditis—inflammation of the heart. Some of these cases resolve on their own, but others cause persistent scarring, and still others rapidly progress into lethal problems. No one knows what proportion of people with viral myocarditis experience the most mild fate, because doctors typically notice only those who seek medical attention. But now researchers are also intently scrutinizing the hearts of people with mild or asymptomatic COVID‑19 infections, including college athletes, given concerns about sudden cardiac arrest during strenuous workouts. The lessons from these efforts could ultimately avert deaths from other infections.
Respiratory viruses, though extremely common, are often neglected. Respiratory syncytial virus, parainfluenza viruses, rhinoviruses, adenoviruses, bocaviruses, a quartet of other human coronaviruses—they mostly cause mild coldlike illnesses, but those can be severe. How often? Why? It’s hard to say, because, influenza aside, such viruses attract little funding or interest. “There’s a perception that they’re just colds and there’s nothing much to learn,” says Emily Martin of the University of Michigan, who has long struggled to get funding to study them. Such reasoning is shortsighted folly. Respiratory viruses are the pathogens most likely to cause pandemics, and those outbreaks could potentially be far worse than COVID‑19’s.
Read: We need to talk about ventilation
Their movements through the air have been poorly studied, too. “There’s this very entrenched idea,” says Linsey Marr at Virginia Tech, that viruses mostly spread through droplets (short-range globs of snot and spit) rather than aerosols (smaller, dustlike flecks that travel farther). That idea dates back to the 1930s, when scientists were upending outdated notions that disease was caused by “bad air,” or miasma. But the evidence that SARS‑CoV‑2 can spread through aerosols “is now overwhelming,” says Marr, one of the few scientists who, before the pandemic, studied how viruses spread through air. “I’ve seen more acceptance in the last six months than over the 12 years I’ve been working on this.”
Another pandemic is inevitable, but it will find a very different community of scientists than COVID‑19 did. They will immediately work to determine whether the pathogen—most likely another respiratory virus—moves through aerosols, and whether it spreads from infected people before causing symptoms. They might call for masks and better ventilation from the earliest moments, not after months of debate. They will anticipate the possibility of an imminent wave of long-haul symptoms, and hopefully discover ways of preventing them. They might set up research groups to prioritize the most promising drugs and coordinate large clinical trials. They might take vaccine platforms that worked best against COVID‑19, slot in the genetic material of the new pathogen, and have a vaccine ready within months.
For all its benefits, the single-minded focus on COVID‑19 will also leave a slew of negative legacies. Science is mostly a zero-sum game, and when one topic monopolizes attention and money, others lose out. Last year, between physical-distancing restrictions, redirected funds, and distracted scientists, many lines of research slowed to a crawl. Long-term studies that monitored bird migrations or the changing climate will forever have holes in their data because field research had to be canceled. Conservationists who worked to protect monkeys and apes kept their distance for fear of passing COVID‑19 to already endangered species. Roughly 80 percent of non-COVID‑19 clinical trials in the U.S.—likely worth billions of dollars—were interrupted or stopped because hospitals were overwhelmed and volunteers were stuck at home. Even research on other infectious diseases was back-burnered. “All the non-COVID work that I was working on before the pandemic started is now piling up and gathering dust,” says Angela Rasmussen of Georgetown University, who normally studies Ebola and MERS. “Those are still problems.”
The COVID‑19 pandemic is a singular disaster, and it is reasonable for society—and scientists—to prioritize it. But the pivot was driven by opportunism as much as altruism. Governments, philanthropies, and universities channeled huge sums toward COVID‑19 research. The NIH alone received nearly $3.6 billion from Congress. The Bill & Melinda Gates Foundation apportioned $350 million for COVID‑19 work. “Whenever there’s a big pot of money, there’s a feeding frenzy,” Madhukar Pai told me. He works on tuberculosis, which causes 1.5 million deaths a year—comparable to COVID‑19’s toll in 2020. Yet tuberculosis research has been mostly paused. None of Pai’s colleagues pivoted when Ebola or Zika struck, but “half of us have now swung to working on COVID‑19,” he said. “It’s a black hole, sucking us all in.”
While the most qualified experts became quickly immersed in the pandemic response, others were stuck at home looking for ways to contribute. Using the same systems that made science faster, they could download data from free databases, run quick analyses with intuitive tools, publish their work on preprint servers, and publicize it on Twitter. Often, they made things worse by swerving out of their scholarly lanes and plowing into unfamiliar territory. Nathan Ballantyne, a philosopher at Fordham University, calls this “ epistemic trespassing .” It can be a good thing: Continental drift was championed by Alfred Wegener, a meteorologist; microbes were first documented by Antonie van Leeuwenhoek, a draper. But more often than not, epistemic trespassing just creates a mess, especially when inexperience couples with overconfidence.
On March 28, a preprint noted that countries that universally use a tuberculosis vaccine called BCG had lower COVID‑19 mortality rates. But such cross-country comparisons are infamously treacherous. For example, countries with higher cigarette-usage rates have longer life expectancies, not because smoking prolongs life but because it is more popular in wealthier nations. This tendency to draw faulty conclusions about individual health using data about large geographical regions is called the ecological fallacy. Epidemiologists know to avoid it. The BCG-preprint authors, who were from an osteopathic college in New York, didn’t seem to . But their paper was covered by more than 70 news outlets, and dozens of inexperienced teams offered similarly specious analyses. “People who don’t know how to spell tuberculosis have told me they can solve the link between BCG and COVID‑19,” Pai said. “Someone told me they can do it in 48 hours with a hackathon.”

Other epistemic trespassers spent their time reinventing the wheel. One new study, published in NEJM , used lasers to show that when people speak, they release aerosols. But as the authors themselves note, the same result—sans lasers—was published in 1946, Marr says. I asked her whether any papers from the 2020 batch had taught her something new. After an uncomfortably long pause, she mentioned just one.
In some cases, bad papers helped shape the public narrative of the pandemic. On March 16, two biogeographers published a preprint arguing that COVID‑19 will “marginally affect the tropics” because it fares poorly in warm, humid conditions. Disease experts quickly noted that techniques like the ones the duo used are meant for modeling the geographic ranges of animal and plant species or vector-borne pathogens, and are ill-suited to simulating the spread of viruses like SARS-CoV-2. But their claim was picked up by more than 50 news outlets and echoed by the United Nations World Food Program. COVID‑19 has since run rampant in many tropical countries, including Brazil, Indonesia, and Colombia—and the preprint’s authors have qualified their conclusions in later versions of the paper. “It takes a certain type of person to think that weeks of reading papers gives them more perspective than someone with a Ph.D. on that subject, and that type of person has gotten a lot of airtime in this pandemic,” says Colin Carlson of Georgetown.
The incentives to trespass are substantial. Academia is a pyramid scheme: Each biomedical professor trains an average of six doctoral students across her career, but only 16 percent of the students get tenure-track positions . Competition is ferocious, and success hinges on getting published—a feat made easier by dramatic results. These factors pull researchers toward speed, short-termism, and hype at the expense of rigor—and the pandemic intensified that pull. With an anxious world crying out for information, any new paper could immediately draw international press coverage—and hundreds of citations.
The tsunami of rushed but dubious work made life harder for actual experts, who struggled to sift the signal from the noise. They also felt obliged to debunk spurious research in long Twitter threads and relentless media interviews—acts of public service that are rarely rewarded in academia. And they were overwhelmed by requests to peer-review new papers. Kristian Andersen, an infectious-disease researcher at Scripps Research, told me that journals used to send him two or three such requests a month. Now “I’m getting three or five a day,” he said in September.
The pandemic’s opportunities also fell inequitably upon the scientific community. In March, Congress awarded $75 million to the National Science Foundation to fast-track studies that could quickly contribute to the pandemic response. “That money just went ,” says Cassidy Sugimoto of Indiana University, who was on rotation at the agency at the time. “It was a first-come, first-served environment. It advantaged people who were aware of the system and could act upon it quickly.” But not all scientists could pivot to COVID‑19, or pivot with equal speed.
Among scientists, as in other fields, women do more child care, domestic work, and teaching than men, and are more often asked for emotional support by their students. These burdens increased as the pandemic took hold, leaving women scientists “less able to commit their time to learning about a new area of study, and less able to start a whole new research project,” says Molly M. King, a sociologist at Santa Clara University. Women’s research hours fell by nine percentage points more than did men’s because of the pressures of COVID‑19. And when COVID‑19 created new opportunities, men grabbed them more quickly. In the spring, the proportion of papers with women as first authors fell almost 44 percent in the preprint repository medRxiv, relative to 2019. And published COVID‑19 papers had 19 percent fewer women as first authors compared with papers from the same journals in the previous year. Men led more than 80 percent of national COVID‑19 task forces in 87 countries . Male scientists were quoted four times as frequently as female scientists in American news stories about the pandemic.
American scientists of color also found it harder to pivot than their white peers, because of unique challenges that sapped their time and energy. Black, Latino, and Indigenous scientists were most likely to have lost loved ones, adding mourning to their list of duties. Many grieved, too, after the killings of Breonna Taylor, George Floyd, Ahmaud Arbery, and others. They often faced questions from relatives who were mistrustful of the medical system, or were experiencing discriminatory care. They were suddenly tasked with helping their predominantly white institutions fight racism. Neil Lewis Jr. at Cornell, who studies racial health disparities, told me that many psychologists had long deemed his work irrelevant. “All of a sudden my inbox is drowning,” he said, while some of his own relatives have become ill and one has died.
Science suffers from the so-called Matthew effect, whereby small successes snowball into ever greater advantages, irrespective of merit. Similarly, early hindrances linger. Young researchers who could not pivot because they were too busy caring or grieving for others might suffer lasting consequences from an unproductive year. COVID‑19 “has really put the clock back in terms of closing the gap for women and underrepresented minorities,” Yale’s Akiko Iwasaki says. “Once we’re over the pandemic, we’ll need to fix it all again.”
COVID-19 has already changed science immensely, but if scientists are savvy, the most profound pivot is still to come—a grand reimagining of what medicine should be. In 1848, the Prussian government sent a young physician named Rudolf Virchow to investigate a typhus epidemic in Upper Silesia. Virchow didn’t know what caused the devastating disease, but he realized its spread was possible because of malnutrition, hazardous working conditions, crowded housing, poor sanitation, and the inattention of civil servants and aristocrats—problems that require social and political reforms. “Medicine is a social science,” Virchow said, “and politics is nothing but medicine in larger scale.”
This viewpoint fell by the wayside after germ theory became mainstream in the late 19th century. When scientists discovered the microbes responsible for tuberculosis, plague, cholera, dysentery, and syphilis, most fixated on these newly identified nemeses. Societal factors were seen as overly political distractions for researchers who sought to “be as ‘objective’ as possible,” says Elaine Hernandez, a medical sociologist at Indiana University. In the U.S., medicine fractured. New departments of sociology and cultural anthropology kept their eye on the societal side of health, while the nation’s first schools of public health focused instead on fights between germs and individuals. This rift widened as improvements in hygiene, living standards, nutrition, and sanitation lengthened life spans: The more social conditions improved, the more readily they could be ignored.
The ideological pivot away from social medicine began to reverse in the second half of the 20th century. The women’s-rights and civil-rights movements, the rise of environmentalism, and anti-war protests created a generation of scholars who questioned “the legitimacy, ideology, and practice of any science … that disregards social and economic inequality,” wrote Nancy Krieger of Harvard . Beginning in the 1980s, this new wave of social epidemiologists once again studied how poverty, privilege, and living conditions affect a person’s health—to a degree even Virchow hadn’t imagined. But as COVID‑19 has shown, the reintegration is not yet complete.
Politicians initially described COVID‑19 as a “great equalizer,” but when states began releasing demographic data, it was immediately clear that the disease was disproportionately infecting and killing people of color . These disparities aren’t biological. They stem from decades of discrimination and segregation that left minority communities in poorer neighborhoods with low-paying jobs, more health problems, and less access to health care—the same kind of problems that Virchow identified more than 170 years ago.
From the September 2020 issue: How the pandemic defeated America
Simple acts like wearing a mask and staying at home, which rely on people tolerating discomfort for the collective good, became society’s main defenses against the virus in the many months without effective drugs or vaccines. These are known as nonpharmaceutical interventions—a name that betrays medicine’s biological bias. For most of 2020, these were the only interventions on offer, but they were nonetheless defined in opposition to the more highly prized drugs and vaccines.
In March, when the U.S. started shutting down, one of the biggest questions on the mind of Whitney Robinson of UNC at Chapel Hill was: Are our kids going to be out of school for two years? While biomedical scientists tend to focus on sickness and recovery, social epidemiologists like her “think about critical periods that can affect the trajectory of your life,” she told me. Disrupting a child’s schooling at the wrong time can affect their entire career, so scientists should have prioritized research to figure out whether and how schools could reopen safely. But most studies on the spread of COVID‑19 in schools were neither large in scope nor well-designed enough to be conclusive. No federal agency funded a large, nationwide study, even though the federal government had months to do so. The NIH received billions for COVID‑19 research , but the National Institute of Child Health and Human Development—one of its 27 constituent institutes and centers—got nothing.
The horrors that Rudolf Virchow saw in Upper Silesia radicalized him, pushing the future “father of modern pathology” to advocate for social reforms. The current pandemic has affected scientists in the same way. Calm researchers became incensed as potentially game-changing innovations like cheap diagnostic tests were squandered by a negligent administration and a muzzled Centers for Disease Control and Prevention. Austere publications like NEJM and Nature published explicitly political editorials castigating the Trump administration for its failures and encouraging voters to hold the president accountable. COVID‑19 could be the catalyst that fully reunifies the social and biological sides of medicine, bridging disciplines that have been separated for too long.
“To study COVID‑19 is not only to study the disease itself as a biological entity,” says Alondra Nelson, the president of the Social Science Research Council. “What looks like a single problem is actually all things, all at once. So what we’re actually studying is literally everything in society, at every scale, from supply chains to individual relationships.”
The scientific community spent the pre-pandemic years designing faster ways of doing experiments, sharing data, and developing vaccines, allowing it to mobilize quickly when COVID‑19 emerged. Its goal now should be to address its many lingering weaknesses. Warped incentives, wasteful practices, overconfidence, inequality, a biomedical bias—COVID‑19 has exposed them all. And in doing so, it offers the world of science a chance to practice one of its most important qualities: self-correction.
* The print version of this article stated that the Moderna and Pfizer/BioNTech vaccines were reported to be 95 percent effective at preventing COVID-19 infections. In fact, the vaccines prevent disease, not infection.
This article appears in the January/February 2021 print edition with the headline “The COVID-19 Manhattan Project.”

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Advanced Search
- Journal List
- Methodist Debakey Cardiovasc J
- v.17(5); 2021
The Way Ahead: Life After COVID-19
Mouaz h. al-mallah.
1 Houston Methodist DeBakey Heart & Vascular Center, Houston, TX, US
Much has changed in the 2 years since the start of the coronavirus disease 19 (COVID-19) pandemic. The need for social distancing catalyzed the digitization of healthcare delivery and medical education—from telemedicine and virtual conferences to online residency/fellowship interviews. Vaccine development, particularly in the field of mRNA technology, led to widespread availability of safe and effective vaccines. With improved survival from acute infection, the healthcare system is dealing with the ever-growing cohort of patients with lingering symptoms. In addition, social media platforms have fueled a plethora of misinformation campaigns that have adversely affected prevention and control measures. In this review, we examine how COVID-19 has reshaped the healthcare system, and gauge its potential effects on life after the pandemic.
Introduction
In December 2021, after many months of living with the COVID-19 pandemic, the world is still looking for a way out of this healthcare crisis. As of this writing, more than 250 million people globally have been infected with SARS-CoV-2, the virus that causes coronavirus disease 19 (COVID-19), and nearly 5 million individuals lost their lives battling the complications of severe acute respiratory syndromes. 1 Many communities experienced multiple surges of the virus, with changes in normal life and restrictions to daily activities. The intensification of vaccination efforts brought about hope for a possible end to the pandemic. However, the continued emergence of variant strains and vaccine hesitancy have been persistent challenges in the US and globally. In this article, we review the long-term effect of COVID-19 on healthcare systems and envision the future of life after the pandemic ( Figure 1 ).
")
The long-term effects of the coronavirus disease 19 (COVID-19) pandemic on the healthcare system.
Since the beginning of the pandemic, there have been accelerated efforts to sequence the genetic material of the virus and build effective vaccines that decrease the risk of infection, hospitalization, and mortality. 2 At the time of this writing, more than 10 vaccines have been approved by local healthcare authorities in different parts of the world. 3 The pandemic has also driven innovation in the novel field of messenger ribonucleic acid (mRNA) vaccines. The US Food and Drug Administration (FDA) has approved the use of the Pfizer-BioNTech mRNA vaccine and given emergency use authorization to Moderna. 4 The mRNA vaccines have shown excellent efficacy against many of the strains, including the beta and delta strains.
More recently, booster doses have been approved by the FDA for individuals aged 65 years and older as well as individuals with comorbidities, in long-term care facilities, or at increased risk for COVID-19 exposure and transmission due to occupational or institutional settings. 5 Furthermore, the FDA has also given emergency use authorization for the Pfizer-BioNTech vaccine in individuals aged 12 to 17 years and, as of October 29, in children aged 5 to 11 years.
Although the fast-tracked vaccine production time led some skeptics to hypothesize safety concerns, the rate of adverse events has been very low. One complication that gained significant attention is myocarditis. 6 , 7 , 8 Emerging data have shown that young men are the most commonly affected demographic. Furthermore, the risk was elevated in the setting of a recent COVID-19 illness and after the second dose of the vaccine. 6 , 7 Although the rate of myocarditis is low and the majority of patients recover, the risk of recurrence in patients who developed myocarditis with the first dose or in patients with recent myocarditis is unclear. Similarly, the rate of recurrence after the second or booster doses also is unclear.
Vaccine Mandates
Multiple state and federal governments have issued vaccine mandates, and they have become a highly contested political issue in the United States. The Biden administration issued an executive order on September 9, 2021, requiring all federal employees to vaccinate. 9 Some state and local governments have also followed. 10
Multiple US healthcare systems have also issued COVID-19 vaccine mandates for employees. On March 31, 2021, Houston Methodist became the first healthcare system to mandate the vaccine for employees, and a wave of other healthcare systems followed suit. 11 As of this writing, more than 2,500 hospitals or health systems have followed Houston Methodist and mandated vaccines for their clinical and nonclinical staff. 12
Combating Misinformation
Since the beginning of the pandemic, misinformation has spread throughout the Internet and on social media platforms. 13 People have questioned the existence of the virus, the strain on healthcare systems, and the benefit of masks as well as emphasized the benefits of unproven therapies, many of which were useless and even harmful. 14 Political agendas have also played into the misinformation campaigns. Studies have shown that these misinformation campaigns have had measurable effects on the intent to vaccinate and created widespread fear and panic, ultimately contributing to the reduced number of people willing to vaccinate. 13 , 15 , 16 Tackling this will require concerted efforts by the government and private sector, particularly social media companies, to implement evidence-based communication strategies. 17 Individuals should also assume responsibility in seeking out accurate, evidence-based information for their own consumption.
Telemedicine
As many states and cities implemented measures to reduce transmission, telehealth emerged as the ideal tool to continue patient care while protecting the health of both patients and providers. Many patients preferred this option, especially when hospitals were dealing with record numbers of COVID-19 infections. In 2020, telemedicine was the main means by which ambulatory care was provided, accounting for 10% to 20% of visits when virus transmissibility was low and as high as 80% of visits during the surges. 18
Accordingly, the US Department of Health and Human Services relaxed enforcement of software-based Health Insurance Portability and Accountability Act violations, the Centers for Medicaid and Medicare Services provided waivers for telehealth reimbursements, and, in many instances, commercial insurances provided the same either directly or through mandates provided by local state governments. 19 , 20 The removal of regulatory and reimbursement barriers led to a dramatic increase in the use of telehealth, with some institutions reporting multifold increase in telehealth visits. 21
The pandemic also served as a catalyst for innovation in the software and hardware necessary for telemedicine. 22 For example, important tools were developed to enable secure connections with physicians and allow remote vital sign and weight monitoring. 23 , 24 Unfortunately, not all have equally benefitted from the expanded use of telehealth. Data indicate that minorities and disadvantaged groups often lack access to telehealth-based care. 25 Although the positive response and uptake by physicians and patients indicates the likelihood of telemedicine continuing past the pandemic, it remains to be seen whether the regulatory and reimbursement aspects will continue.
Post Covid-19 Condition
There is a growing body of evidence that some patients have prolonged recovery and/or residual symptoms after acute infection with COVID-19. The World Health Organization has defined this as “post COVID-19 condition.” Common presentation includes shortness of breath, palpitation, anxiety, and depression lingering for several months after acute infection. 26 , 27 Recent data also suggests that post COVID-19 condition might not be limited to somatic symptoms, with studies showing a 7-fold increased risk of developing depression and mental health issues. 28
Although the cause of these symptoms is not clear, one possible link that partly explains the prolonged shortness of breath experienced by some patients is COVID-19–associated myocarditis and the associated microvascular dysfunction. 26 As the pandemic continues and therapeutics improve survival from acute infection, the number of patients reporting post COVID-19 condition is predicted to grow. Several medical centers have already established clinics to better coordinate care and conduct research on the long-term impact and treatment of COVID-19. 29
Collateral Damage
Many patients delayed regular and preventive care during the pandemic due to fear of contracting COVID-19. 30 , 31 Such change in health-seeking behavior also extended to emergency conditions, with studies showing how some patients did not seek care for new onset chest pain. 32 Indirect indicators of this are the reduced rates of cardiovascular testing globally and within the United States 33 , 34 and the increased rate of myocardial infarctions and other emergencies seen on the trailing end of COVID-19–infection surges. 32 There has also been an increase in late complications of myocardial infarction such as ventricular septal rupture, a rare occurrence in the prepandemic reperfusion era and one partly explained by delayed care and ignored early warning signs. 35
Disparities in Healthcare
The pandemic exposed significant disparities in healthcare delivery, particularly among minorities. They were more likely to be affected by misinformation campaigns and less likely to accept research supporting clinical therapies and vaccines. Understanding the disparities and identifying measures to bridge the gap will be an important area of research for policy.
Globally, the pandemic also exposed significant inequities regarding vaccine access. While many developed countries were able to reach vaccination rates as high as 70%, rates in low-to-middle-income countries have remained low. 35 As the delta variant has clearly shown, no one is safe until everyone is safe. To this end, the World Health Organization and the COVAX (COVID-19 Vaccines Global Access) alliance have been a vital source of affordable vaccines. 36
Changes to Medical Education
The pandemic resulted in significant changes to both graduate and continued medical education. Much like patient-physician encounters, postgraduate training programs limited large face-to-face gatherings and transitioned all teaching to online platforms. 37 Residency and fellowship recruitment interviews also shifted to online settings. Lastly, there has been an exponential increase in the number of continued medical education offerings, with many societal meetings and conferences transitioning to online or hybrid formats. 38
The medical community has, for the most part, been very receptive to these changes, and it has afforded unforeseen advantages to trainees. Residency and fellowship applicants no longer need to bear the logistic and financial burden of in-person interviews. More importantly, virtual meetings and conferences have significantly increased audiences and, by extension, enabled the wider dissemination of medical knowledge.
The COVID-19 pandemic has dramatically changed clinical practice, medical education, and research. Beyond the immediate increase in morbidity and mortality, the healthcare system is having to deal with a growing cohort of patients with lingering symptoms. Misinformation, vaccine hesitancy, and vaccine inequity will be continuing challenges to attaining herd immunity. Clinicians, educators, and healthcare administrators will also have to determine how best to leverage the transition to virtual platforms. Lastly, healthcare leaders and policy makers will have to help the country and world chart a course through the end of the pandemic.
- The coronavirus disease 19 (COVID-19) pandemic has dramatically changed clinical practice, medical education, and research.
- It has brought about new challenges for the healthcare system, such as how best to combat misinformation, address the disproportionate impact on minorities and marginalized groups, and treat the ever-growing population of patients with lingering “long COVID” symptoms.
- The pandemic has also catalyzed much needed change in vaccine development, telemedicine, and medical education.
- Addressing these challenges and charting a way forward will require the concerted effort of clinicians, healthcare leaders, and policy makers.
Competing Interests
Dr. Al-Mallah has completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Volume 76, Issue 2
- COVID-19 pandemic and its impact on social relationships and health
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0000-0003-1512-4471 Emily Long 1 ,
- Susan Patterson 1 ,
- Karen Maxwell 1 ,
- Carolyn Blake 1 ,
- http://orcid.org/0000-0001-7342-4566 Raquel Bosó Pérez 1 ,
- Ruth Lewis 1 ,
- Mark McCann 1 ,
- Julie Riddell 1 ,
- Kathryn Skivington 1 ,
- Rachel Wilson-Lowe 1 ,
- http://orcid.org/0000-0002-4409-6601 Kirstin R Mitchell 2
- 1 MRC/CSO Social and Public Health Sciences Unit , University of Glasgow , Glasgow , UK
- 2 MRC/CSO Social and Public Health Sciences Unit, Institute of Health & Wellbeing , University of Glasgow , Glasgow , UK
- Correspondence to Dr Emily Long, MRC/CSO Social and Public Health Sciences Unit, University of Glasgow, Glasgow G3 7HR, UK; emily.long{at}glasgow.ac.uk
This essay examines key aspects of social relationships that were disrupted by the COVID-19 pandemic. It focuses explicitly on relational mechanisms of health and brings together theory and emerging evidence on the effects of the COVID-19 pandemic to make recommendations for future public health policy and recovery. We first provide an overview of the pandemic in the UK context, outlining the nature of the public health response. We then introduce four distinct domains of social relationships: social networks, social support, social interaction and intimacy, highlighting the mechanisms through which the pandemic and associated public health response drastically altered social interactions in each domain. Throughout the essay, the lens of health inequalities, and perspective of relationships as interconnecting elements in a broader system, is used to explore the varying impact of these disruptions. The essay concludes by providing recommendations for longer term recovery ensuring that the social relational cost of COVID-19 is adequately considered in efforts to rebuild.
- inequalities
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study. Data sharing not applicable as no data sets generated or analysed for this essay.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/ .
https://doi.org/10.1136/jech-2021-216690
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Introduction
Infectious disease pandemics, including SARS and COVID-19, demand intrapersonal behaviour change and present highly complex challenges for public health. 1 A pandemic of an airborne infection, spread easily through social contact, assails human relationships by drastically altering the ways through which humans interact. In this essay, we draw on theories of social relationships to examine specific ways in which relational mechanisms key to health and well-being were disrupted by the COVID-19 pandemic. Relational mechanisms refer to the processes between people that lead to change in health outcomes.
At the time of writing, the future surrounding COVID-19 was uncertain. Vaccine programmes were being rolled out in countries that could afford them, but new and more contagious variants of the virus were also being discovered. The recovery journey looked long, with continued disruption to social relationships. The social cost of COVID-19 was only just beginning to emerge, but the mental health impact was already considerable, 2 3 and the inequality of the health burden stark. 4 Knowledge of the epidemiology of COVID-19 accrued rapidly, but evidence of the most effective policy responses remained uncertain.
The initial response to COVID-19 in the UK was reactive and aimed at reducing mortality, with little time to consider the social implications, including for interpersonal and community relationships. The terminology of ‘social distancing’ quickly became entrenched both in public and policy discourse. This equation of physical distance with social distance was regrettable, since only physical proximity causes viral transmission, whereas many forms of social proximity (eg, conversations while walking outdoors) are minimal risk, and are crucial to maintaining relationships supportive of health and well-being.
The aim of this essay is to explore four key relational mechanisms that were impacted by the pandemic and associated restrictions: social networks, social support, social interaction and intimacy. We use relational theories and emerging research on the effects of the COVID-19 pandemic response to make three key recommendations: one regarding public health responses; and two regarding social recovery. Our understanding of these mechanisms stems from a ‘systems’ perspective which casts social relationships as interdependent elements within a connected whole. 5
Social networks
Social networks characterise the individuals and social connections that compose a system (such as a workplace, community or society). Social relationships range from spouses and partners, to coworkers, friends and acquaintances. They vary across many dimensions, including, for example, frequency of contact and emotional closeness. Social networks can be understood both in terms of the individuals and relationships that compose the network, as well as the overall network structure (eg, how many of your friends know each other).
Social networks show a tendency towards homophily, or a phenomenon of associating with individuals who are similar to self. 6 This is particularly true for ‘core’ network ties (eg, close friends), while more distant, sometimes called ‘weak’ ties tend to show more diversity. During the height of COVID-19 restrictions, face-to-face interactions were often reduced to core network members, such as partners, family members or, potentially, live-in roommates; some ‘weak’ ties were lost, and interactions became more limited to those closest. Given that peripheral, weaker social ties provide a diversity of resources, opinions and support, 7 COVID-19 likely resulted in networks that were smaller and more homogenous.
Such changes were not inevitable nor necessarily enduring, since social networks are also adaptive and responsive to change, in that a disruption to usual ways of interacting can be replaced by new ways of engaging (eg, Zoom). Yet, important inequalities exist, wherein networks and individual relationships within networks are not equally able to adapt to such changes. For example, individuals with a large number of newly established relationships (eg, university students) may have struggled to transfer these relationships online, resulting in lost contacts and a heightened risk of social isolation. This is consistent with research suggesting that young adults were the most likely to report a worsening of relationships during COVID-19, whereas older adults were the least likely to report a change. 8
Lastly, social connections give rise to emergent properties of social systems, 9 where a community-level phenomenon develops that cannot be attributed to any one member or portion of the network. For example, local area-based networks emerged due to geographic restrictions (eg, stay-at-home orders), resulting in increases in neighbourly support and local volunteering. 10 In fact, research suggests that relationships with neighbours displayed the largest net gain in ratings of relationship quality compared with a range of relationship types (eg, partner, colleague, friend). 8 Much of this was built from spontaneous individual interactions within local communities, which together contributed to the ‘community spirit’ that many experienced. 11 COVID-19 restrictions thus impacted the personal social networks and the structure of the larger networks within the society.
Social support
Social support, referring to the psychological and material resources provided through social interaction, is a critical mechanism through which social relationships benefit health. In fact, social support has been shown to be one of the most important resilience factors in the aftermath of stressful events. 12 In the context of COVID-19, the usual ways in which individuals interact and obtain social support have been severely disrupted.
One such disruption has been to opportunities for spontaneous social interactions. For example, conversations with colleagues in a break room offer an opportunity for socialising beyond one’s core social network, and these peripheral conversations can provide a form of social support. 13 14 A chance conversation may lead to advice helpful to coping with situations or seeking formal help. Thus, the absence of these spontaneous interactions may mean the reduction of indirect support-seeking opportunities. While direct support-seeking behaviour is more effective at eliciting support, it also requires significantly more effort and may be perceived as forceful and burdensome. 15 The shift to homeworking and closure of community venues reduced the number of opportunities for these spontaneous interactions to occur, and has, second, focused them locally. Consequently, individuals whose core networks are located elsewhere, or who live in communities where spontaneous interaction is less likely, have less opportunity to benefit from spontaneous in-person supportive interactions.
However, alongside this disruption, new opportunities to interact and obtain social support have arisen. The surge in community social support during the initial lockdown mirrored that often seen in response to adverse events (eg, natural disasters 16 ). COVID-19 restrictions that confined individuals to their local area also compelled them to focus their in-person efforts locally. Commentators on the initial lockdown in the UK remarked on extraordinary acts of generosity between individuals who belonged to the same community but were unknown to each other. However, research on adverse events also tells us that such community support is not necessarily maintained in the longer term. 16
Meanwhile, online forms of social support are not bound by geography, thus enabling interactions and social support to be received from a wider network of people. Formal online social support spaces (eg, support groups) existed well before COVID-19, but have vastly increased since. While online interactions can increase perceived social support, it is unclear whether remote communication technologies provide an effective substitute from in-person interaction during periods of social distancing. 17 18 It makes intuitive sense that the usefulness of online social support will vary by the type of support offered, degree of social interaction and ‘online communication skills’ of those taking part. Youth workers, for instance, have struggled to keep vulnerable youth engaged in online youth clubs, 19 despite others finding a positive association between amount of digital technology used by individuals during lockdown and perceived social support. 20 Other research has found that more frequent face-to-face contact and phone/video contact both related to lower levels of depression during the time period of March to August 2020, but the negative effect of a lack of contact was greater for those with higher levels of usual sociability. 21 Relatedly, important inequalities in social support exist, such that individuals who occupy more socially disadvantaged positions in society (eg, low socioeconomic status, older people) tend to have less access to social support, 22 potentially exacerbated by COVID-19.
Social and interactional norms
Interactional norms are key relational mechanisms which build trust, belonging and identity within and across groups in a system. Individuals in groups and societies apply meaning by ‘approving, arranging and redefining’ symbols of interaction. 23 A handshake, for instance, is a powerful symbol of trust and equality. Depending on context, not shaking hands may symbolise a failure to extend friendship, or a failure to reach agreement. The norms governing these symbols represent shared values and identity; and mutual understanding of these symbols enables individuals to achieve orderly interactions, establish supportive relationship accountability and connect socially. 24 25
Physical distancing measures to contain the spread of COVID-19 radically altered these norms of interaction, particularly those used to convey trust, affinity, empathy and respect (eg, hugging, physical comforting). 26 As epidemic waves rose and fell, the work to negotiate these norms required intense cognitive effort; previously taken-for-granted interactions were re-examined, factoring in current restriction levels, own and (assumed) others’ vulnerability and tolerance of risk. This created awkwardness, and uncertainty, for example, around how to bring closure to an in-person interaction or convey warmth. The instability in scripted ways of interacting created particular strain for individuals who already struggled to encode and decode interactions with others (eg, those who are deaf or have autism spectrum disorder); difficulties often intensified by mask wearing. 27
Large social gatherings—for example, weddings, school assemblies, sporting events—also present key opportunities for affirming and assimilating interactional norms, building cohesion and shared identity and facilitating cooperation across social groups. 28 Online ‘equivalents’ do not easily support ‘social-bonding’ activities such as singing and dancing, and rarely enable chance/spontaneous one-on-one conversations with peripheral/weaker network ties (see the Social networks section) which can help strengthen bonds across a larger network. The loss of large gatherings to celebrate rites of passage (eg, bar mitzvah, weddings) has additional relational costs since these events are performed by and for communities to reinforce belonging, and to assist in transitioning to new phases of life. 29 The loss of interaction with diverse others via community and large group gatherings also reduces intergroup contact, which may then tend towards more prejudiced outgroup attitudes. While online interaction can go some way to mimicking these interaction norms, there are key differences. A sense of anonymity, and lack of in-person emotional cues, tends to support norms of polarisation and aggression in expressing differences of opinion online. And while online platforms have potential to provide intergroup contact, the tendency of much social media to form homogeneous ‘echo chambers’ can serve to further reduce intergroup contact. 30 31
Intimacy relates to the feeling of emotional connection and closeness with other human beings. Emotional connection, through romantic, friendship or familial relationships, fulfils a basic human need 32 and strongly benefits health, including reduced stress levels, improved mental health, lowered blood pressure and reduced risk of heart disease. 32 33 Intimacy can be fostered through familiarity, feeling understood and feeling accepted by close others. 34
Intimacy via companionship and closeness is fundamental to mental well-being. Positively, the COVID-19 pandemic has offered opportunities for individuals to (re)connect and (re)strengthen close relationships within their household via quality time together, following closure of many usual external social activities. Research suggests that the first full UK lockdown period led to a net gain in the quality of steady relationships at a population level, 35 but amplified existing inequalities in relationship quality. 35 36 For some in single-person households, the absence of a companion became more conspicuous, leading to feelings of loneliness and lower mental well-being. 37 38 Additional pandemic-related relational strain 39 40 resulted, for some, in the initiation or intensification of domestic abuse. 41 42
Physical touch is another key aspect of intimacy, a fundamental human need crucial in maintaining and developing intimacy within close relationships. 34 Restrictions on social interactions severely restricted the number and range of people with whom physical affection was possible. The reduction in opportunity to give and receive affectionate physical touch was not experienced equally. Many of those living alone found themselves completely without physical contact for extended periods. The deprivation of physical touch is evidenced to take a heavy emotional toll. 43 Even in future, once physical expressions of affection can resume, new levels of anxiety over germs may introduce hesitancy into previously fluent blending of physical and verbal intimate social connections. 44
The pandemic also led to shifts in practices and norms around sexual relationship building and maintenance, as individuals adapted and sought alternative ways of enacting sexual intimacy. This too is important, given that intimate sexual activity has known benefits for health. 45 46 Given that social restrictions hinged on reducing household mixing, possibilities for partnered sexual activity were primarily guided by living arrangements. While those in cohabiting relationships could potentially continue as before, those who were single or in non-cohabiting relationships generally had restricted opportunities to maintain their sexual relationships. Pornography consumption and digital partners were reported to increase since lockdown. 47 However, online interactions are qualitatively different from in-person interactions and do not provide the same opportunities for physical intimacy.
Recommendations and conclusions
In the sections above we have outlined the ways in which COVID-19 has impacted social relationships, showing how relational mechanisms key to health have been undermined. While some of the damage might well self-repair after the pandemic, there are opportunities inherent in deliberative efforts to build back in ways that facilitate greater resilience in social and community relationships. We conclude by making three recommendations: one regarding public health responses to the pandemic; and two regarding social recovery.
Recommendation 1: explicitly count the relational cost of public health policies to control the pandemic
Effective handling of a pandemic recognises that social, economic and health concerns are intricately interwoven. It is clear that future research and policy attention must focus on the social consequences. As described above, policies which restrict physical mixing across households carry heavy and unequal relational costs. These include for individuals (eg, loss of intimate touch), dyads (eg, loss of warmth, comfort), networks (eg, restricted access to support) and communities (eg, loss of cohesion and identity). Such costs—and their unequal impact—should not be ignored in short-term efforts to control an epidemic. Some public health responses—restrictions on international holiday travel and highly efficient test and trace systems—have relatively small relational costs and should be prioritised. At a national level, an earlier move to proportionate restrictions, and investment in effective test and trace systems, may help prevent escalation of spread to the point where a national lockdown or tight restrictions became an inevitability. Where policies with relational costs are unavoidable, close attention should be paid to the unequal relational impact for those whose personal circumstances differ from normative assumptions of two adult families. This includes consideration of whether expectations are fair (eg, for those who live alone), whether restrictions on social events are equitable across age group, religious/ethnic groupings and social class, and also to ensure that the language promoted by such policies (eg, households; families) is not exclusionary. 48 49 Forethought to unequal impacts on social relationships should thus be integral to the work of epidemic preparedness teams.
Recommendation 2: intelligently balance online and offline ways of relating
A key ingredient for well-being is ‘getting together’ in a physical sense. This is fundamental to a human need for intimate touch, physical comfort, reinforcing interactional norms and providing practical support. Emerging evidence suggests that online ways of relating cannot simply replace physical interactions. But online interaction has many benefits and for some it offers connections that did not exist previously. In particular, online platforms provide new forms of support for those unable to access offline services because of mobility issues (eg, older people) or because they are geographically isolated from their support community (eg, lesbian, gay, bisexual, transgender and queer (LGBTQ) youth). Ultimately, multiple forms of online and offline social interactions are required to meet the needs of varying groups of people (eg, LGBTQ, older people). Future research and practice should aim to establish ways of using offline and online support in complementary and even synergistic ways, rather than veering between them as social restrictions expand and contract. Intelligent balancing of online and offline ways of relating also pertains to future policies on home and flexible working. A decision to switch to wholesale or obligatory homeworking should consider the risk to relational ‘group properties’ of the workplace community and their impact on employees’ well-being, focusing in particular on unequal impacts (eg, new vs established employees). Intelligent blending of online and in-person working is required to achieve flexibility while also nurturing supportive networks at work. Intelligent balance also implies strategies to build digital literacy and minimise digital exclusion, as well as coproducing solutions with intended beneficiaries.
Recommendation 3: build stronger and sustainable localised communities
In balancing offline and online ways of interacting, there is opportunity to capitalise on the potential for more localised, coherent communities due to scaled-down travel, homeworking and local focus that will ideally continue after restrictions end. There are potential economic benefits after the pandemic, such as increased trade as home workers use local resources (eg, coffee shops), but also relational benefits from stronger relationships around the orbit of the home and neighbourhood. Experience from previous crises shows that community volunteer efforts generated early on will wane over time in the absence of deliberate work to maintain them. Adequately funded partnerships between local government, third sector and community groups are required to sustain community assets that began as a direct response to the pandemic. Such partnerships could work to secure green spaces and indoor (non-commercial) meeting spaces that promote community interaction. Green spaces in particular provide a triple benefit in encouraging physical activity and mental health, as well as facilitating social bonding. 50 In building local communities, small community networks—that allow for diversity and break down ingroup/outgroup views—may be more helpful than the concept of ‘support bubbles’, which are exclusionary and less sustainable in the longer term. Rigorously designed intervention and evaluation—taking a systems approach—will be crucial in ensuring scale-up and sustainability.
The dramatic change to social interaction necessitated by efforts to control the spread of COVID-19 created stark challenges but also opportunities. Our essay highlights opportunities for learning, both to ensure the equity and humanity of physical restrictions, and to sustain the salutogenic effects of social relationships going forward. The starting point for capitalising on this learning is recognition of the disruption to relational mechanisms as a key part of the socioeconomic and health impact of the pandemic. In recovery planning, a general rule is that what is good for decreasing health inequalities (such as expanding social protection and public services and pursuing green inclusive growth strategies) 4 will also benefit relationships and safeguard relational mechanisms for future generations. Putting this into action will require political will.
Ethics statements
Patient consent for publication.
Not required.
- Office for National Statistics (ONS)
- Ford T , et al
- Riordan R ,
- Ford J , et al
- Glonti K , et al
- McPherson JM ,
- Smith-Lovin L
- Granovetter MS
- Fancourt D et al
- Stadtfeld C
- Office for Civil Society
- Cook J et al
- Rodriguez-Llanes JM ,
- Guha-Sapir D
- Patulny R et al
- Granovetter M
- Winkeler M ,
- Filipp S-H ,
- Kaniasty K ,
- de Terte I ,
- Guilaran J , et al
- Wright KB ,
- Martin J et al
- Gabbiadini A ,
- Baldissarri C ,
- Durante F , et al
- Sommerlad A ,
- Marston L ,
- Huntley J , et al
- Turner RJ ,
- Bicchieri C
- Brennan G et al
- Watson-Jones RE ,
- Amichai-Hamburger Y ,
- McKenna KYA
- Page-Gould E ,
- Aron A , et al
- Pietromonaco PR ,
- Timmerman GM
- Bradbury-Jones C ,
- Mikocka-Walus A ,
- Klas A , et al
- Marshall L ,
- Steptoe A ,
- Stanley SM ,
- Campbell AM
- ↵ (ONS), O.f.N.S., Domestic abuse during the coronavirus (COVID-19) pandemic, England and Wales . Available: https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/articles/domesticabuseduringthecoronaviruscovid19pandemicenglandandwales/november2020
- Rosenberg M ,
- Hensel D , et al
- Banerjee D ,
- Bruner DW , et al
- Bavel JJV ,
- Baicker K ,
- Boggio PS , et al
- van Barneveld K ,
- Quinlan M ,
- Kriesler P , et al
- Mitchell R ,
- de Vries S , et al
Twitter @karenmaxSPHSU, @Mark_McCann, @Rwilsonlowe, @KMitchinGlasgow
Contributors EL and KM led on the manuscript conceptualisation, review and editing. SP, KM, CB, RBP, RL, MM, JR, KS and RW-L contributed to drafting and revising the article. All authors assisted in revising the final draft.
Funding The research reported in this publication was supported by the Medical Research Council (MC_UU_00022/1, MC_UU_00022/3) and the Chief Scientist Office (SPHSU11, SPHSU14). EL is also supported by MRC Skills Development Fellowship Award (MR/S015078/1). KS and MM are also supported by a Medical Research Council Strategic Award (MC_PC_13027).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Read the full text or download the PDF:
- Latest Latest
- The West The West
- Sports Sports
- Opinion Opinion
- Magazine Magazine
COVID-19: What changed in four years since pandemic was announced?

By Lois M. Collins
The world likely wasn’t paying that much attention on March 11, 2020, when the World Health Organization declared already-worrisome COVID-19 a global pandemic. But that coronavirus, SARS-CoV-2, would soon change world economies, business practices and how health care systems and even schools operated. New and repurposed phrases in the U.S. would soon become part of everyday language in coming months: “masking,” “social distancing,” “flatten the curve,” “quarantine” and “remote work.”
COVID-19 would forever change individual families, too, as the death toll climbed into the millions worldwide.
The fourth anniversary of that pandemic declaration this week is a reminder of how it reshaped the world in profound ways. We better understand preparedness and resilience. We witnessed the vital role of science and research. We found more appreciation for public health and health care workers. We figured out that mental health matters. We saw the value of technology for remote work, education and social connection.
We learned a lot about disease spread and building vaccines fast, about lost jobs and opportunities. We also gained insight into social isolation, the nuclear family and how to put one foot in front of another on a very unfamiliar path. It’s a time to look back, review what happened, and then look forward and commit to keep going when crises inevitably come.
Shutting down
The highly contagious virus had already been declared a public health emergency in the U.S. and three big airlines had already suspended flights to mainland China because of the outbreak there. But despite stories about virus-related illness and death in nursing homes on the West Coast and a deadly outbreak on a cruise ship, U.S. news cycles that morning seemed more taken with the previous night’s Democratic primaries, which nudged Joe Biden along the path to presidential nominee, and the sentencing of film producer Harvey Weinstein for his rape and sexual abuse conviction.
Still, WHO Director-General Dr. Tedros Adhanom Ghebreyesus’ words to the media that morning were stark: “In the past two weeks, the number of cases of COVID-19 outside China has increased 13-fold, and the number of affected countries has tripled. There are now more than 118,000 cases in 114 countries, and 4,291 people have lost their lives. Thousands more are fighting for their lives in hospitals. In the days and weeks ahead, we expect to see the number of cases, the number of deaths and the number of affected countries climb even higher.”
The mysterious illness — best course of treatment unknown, details of its origin unclear, how to stop its spread unmapped, symptoms all over the place, no vaccine available — “can be characterized as a pandemic,” Tedros said. A coronavirus first.
Later that day, Tom Hanks announced he and his wife, Rita Wilson, had contracted COVID-19. That night, President Donald Trump addressed the nation regarding COVID-19. And as Deseret News’ Sarah Todd was covering the Utah Jazz vs. Oklahoma City Thunder, officials sent the gathered crowd home on news that Jazz player Rudy Gobert had tested positive. Soon, the whole NBA season was suspended.
Tedros, standing at his podium, reported 81 countries had no cases and you could count those detected in 57 countries on your fingers. There was time, he cajoled, to “change the course of this pandemic.”
That was a Wednesday. By the weekend, employers and schools were sending people home and businesses were closing. Some never reopened.
At the pandemic’s fourth anniversary, Worldometers reports the U.S. has had 111,638,262 confirmed cases of COVID-19, though it’s clearly a major undercount. Most of us told bosses or schools, family or friends if we got COVID, but aren’t in an official tally. There have been 1,217,245 U.S. COVID-19-related deaths as of March 13, 2024. Those numbers include 5,719 deaths in Utah, of its 1,136,008 reported cases. Nationally, the death count includes 25,996 in the Veterans Administration health care system, 2,268 in the Navajo Nation, 689 in the U.S. military, 324 in federal prisons and seven on the Grand Princess cruise ship.
The New York Times this week made the case that the death toll is much worse than indicated. “The Economist magazine keeps a running estimate of excess deaths , defined as the number of deaths above what was expected from pre-Covid trends. The global total is approaching 30 million.”
A new Lancet study reported the average life expectancy globally dropped by 1.6 years during the pandemic′s first two years. Among high-income nations, the U.S. fared especially poorly, with the highest excess mortality rate in 2020 and 2021.
An unmapped journey
The pandemic was so serious in New York City for a while that nurses were borrowed and bodies were sometimes stored in portable morgues. Overall, New York had 7.5 million cases and more than 83,000 deaths. But it wasn’t the hardest-hit state. Per Worldometers’ statistics, that was California, with 12.7 million cases and more than 112,000 deaths.
Schools went online. Airlines stopped flying to certain countries. re banned entry of noncitizens who had visited 26 different European countries within two weeks of arriving in the U.S. Millions of workers were sent home unless their in-person presence was deemed essential. And the government responded with stimulus money, financial aid for businesses and other help to reduce potential for an economic meltdown.

Two months after the pandemic declaration, Deseret News did an in-depth story on a Grantsville, Utah, husband and father of four, Justin Christensen, then 42, who had been hospitalized for more than two months after becoming sick with COVID-19 on a family trip to Disneyland. For most of that time, he was gravely ill and doctors at University Hospital described feeling their way along a basically uncharted treatment path to save him. They succeeded.
“Doctors are still figuring out how to treat the disease, which has no proven cure. The challenge is great because COVID-19 attacks patients differently; care varies even from room to room in the same hospital. It’s still largely a matter of managing each complication that arises. As the Christensens were about to find out, COVID-19 can change quickly from a distant news story to a battle for survival,” the 2020 article said.
Doctors nationwide were using therapies proven for other illnesses, sometimes boosted by experimental treatments like hydroxychloroquine, described as an “antimalarial long shot” that fell from favor for COVID-19. Though most cases had relatively minor symptoms, so many people needed critical care that they quickly outpaced available medical equipment. States, including Utah, drew up crisis standards of care guidelines to prioritize who’d access tools like ventilators should such decisions be required.
Shortages complicate COVID
So much happened in a very short time.
The disease seemed to ravage older people, so those 60 and older were told to isolate if they could. Visitors were locked out of assisted living, long-term care facilities and hospitals. Families were told to avoid group gatherings and especially older relatives. In a world that needed comfort, hugging and even handshakes stopped.
Meanwhile, local health departments were taking on additional staff to help with contact tracing and governments and public health experts made backup plans as case counts grew. Part of Utah’s backup plan included turning an expo center into a temporary hospital for up to 1,000 patients, complete with a pharmacy.
The pandemic was just two weeks old when Deseret News reported that shortages of lab tests, protective gear and other necessities “have made a severe crisis even worse, with officials begging for help. For example, people who purchased masks, gloves and other protective equipment for personal use early on are asked — along with primary care doctors, veterinarians, dentists, construction workers and others who might have their own supplies of certain types of masks — to donate them to providers for the public good.” Some businesses diverted to manufacture personal protective equipment for health care workers, but even so, non-emergency medical procedures were canceled. With massive need for testing, lines of cars wound into drive-through clinics. Testing supplies and lab capacity was inadequate. In early May, at-home saliva-based testing eased some of the testing angst.
Simple mask designs were created so those who could sew could make their own, even as folks were scouring empty store shelves for toilet paper and hand sanitizer. The entire country learned to obsessively wash their hands while humming the Alphabet Song twice .
Two months feels like eternity when the world shudders. In April, the White House came up with “ gating criteria ” to reopen the economy, based on achieving “benchmarks” reducing illness and deaths, as noted by an American Journal of Managed Care timeline.
In reality, 2020 was a scramble: to make the right public health recommendations, to find the right medicines, to craft better COVID-19 tests, to create vaccines. The latter was actually surprisingly swift , in a government/pharma push nicknamed Operation Warp Speed. As early as May, dozens of vaccine candidates were being considered, including eight already in human trials. By early 2021, three vaccines in the U.S. had fast approval and government contracts for millions of doses.
There were reversals, too. The CDC said masking wouldn’t help. Then everyone was ordered to mask. Experts said the virus spread by touching surfaces, but wasn’t airborne, which it proved to be.
COVID-19 was on a rampage through it all, gathering speed. On June 10, the U.S. hit a 2 million confirmed COVID cases milestone. By Aug. 17, COVID-19 was the No. 3 cause of death in the U.S., behind heart disease and cancer. And each viral mutation brought new degrees of contagion and severity.
Worse, more than a year in, some people couldn’t seem to shake symptoms after surviving the virus. In October 2021, WHO released a clinical definition of “long COVID,” including lingering symptoms. Some are quite serious, including terrible fatigue, brain fog, chronic pain, shortness of breath and chest pain. While not a health catastrophe, losing one’s sense of smell was often cited as a major disappointment.

How COVID-19 changed health care
Health care delivery changed in many ways due to the pandemic, hospitalist Dr. Russell Vinik, chief medical operations officer at University of Utah Healthcare and associate professor of medicine at the U., told Deseret News this week. He thinks some of those changes will last.
Telehealth is a big one. Before the pandemic, visiting with a practitioner by a video link was done primarily for low-acuity urgent care, like a urinary tract infection. Pre-COVID, mental health was also making small inroads in telehealth. But generally, 1 in 100 patient-provider consultations were remote. In the pandemic, it zoomed — literally.
“During the early day in the pandemic, those telehealth systems really weren’t built out to be able to handle it. But we did the best we could so we could take care of patients virtually. What we saw was a very dramatic increase,” he said, noting at least half of patient appointments were telehealth.
That was aided by the fact rules were changed to encourage virtual visits to avoid COVID-19 spread.
While telehealth visits have dropped dramatically to about 1 in 10 or 1 in 12 visits now, they’re certainly no longer 1 in 100. “We’re still probably 10 times higher than what we were pre-pandemic, but significantly lower than those peaks,” Vinik said. And some areas, like mental health, still make robust use of telehealth, maybe as much as 40%, he added. When the care provider doesn’t need to touch the patient, to give an injection or perform a physical exam, care is more amenable to telehealth than when those needs exist.
Masking also changed, Vinik said. “With the exception of maybe our chemotherapy patients, mask utilization was very rare. We’ve learned a lot and I think a lot of us recognize, if I get the sniffles, I should wear a mask. We certainly see a lot more of that now than we did pre-pandemic and I think that’s a good thing.”
He noted that while rules are less restrictive, where patients are the most vulnerable, like neonatal intensive care, “we encourage a lot more mask utilization.” But the culture changed, too. “The pandemic made it somewhat normal and people realize wearing a mask isn’t so terrible.”
Some changes are less welcome, the doctor said, including vaccine skepticism. Even vaccines around for decades may generate skepticism and he noted COVID-19 “propelled an even bigger debate about vaccines,” in part because during the pandemic new methods of making them developed.
One of the tragedies still impacting health is delayed screening. At the height of the pandemic, mammography dropped by over 50%, while colonoscopies fell as much as 80%. The cancers themselves weren’t suspended, just the search for them. So cancers were detected at later stages, Vinik said. “Patients suffered because of that.”
Lessons continue, Vinik said. “We had a pandemic where young, healthy people were dying every day right in front of us. We made the best decisions we could at the time to protect and contain this disease. This is where we learn from it and try to move forward.”
He said we learned “a ton” on the medical side about rapid development of treatments and new tools like mRNA technology that will be helpful in the future. Using antibodies to treat disease was very new and will continue to grow, along with knowledge of how disease propagates.
Failures and sorrow also emerged. “We have this legacy of depression and substance abuse which clearly worsened during the pandemic. It’s really probably too soon to tell if we’re ever going to get back to our pre-pandemic baseline. And we hear all the time about kids that went through junior high and high school, isolated from their friends. How are those kids going to do?” Vinik asked.

Then and now
It’s hard to talk about the pandemic in the U.S. without talking about politics. Pretty early on, political divides erupted centered on COVID-19 policies, probably in part because it was an election year. And some of the division lingers. Even now, folks are divided on vaccines or wearing masks. There are debates about stimulus packages and policies passed when people were losing jobs, businesses and schools were closing and it seemed the economy might rupture. Both liberals and conservatives have criticized the handling of the pandemic.
Liberals say that refusal to be vaccinated led to more spread and more death. Conservatives counter that physically closing schools lowered test scores, which have never recovered. A National Assessment for Educational Progress said that happened in blue states and in red states. COVID-19 clearly disadvantaged school kids.
There’s also pretty broad agreement that a lot was learned, accomplished and managed in a short time. It was all hands on deck: scientists, doctors, politicians, public health, educators, store clerks — name a profession and folks had to step up. Crisis enlivened helpers.
Last May, the public health emergency for COVID-19 ended in the U.S. Just this month, the Centers for Disease Control and Prevention said those who have COVID-19 don’t need to stay in isolation for five days after symptoms leave. We now often talk about COVID-19 like we talk about other more seasonal respiratory viruses. Stories refer to a “tripledemic” that includes influenza, COVID-19 and respiratory syncytial virus, or RSV.
A pain, but no longer a panic.

From the world wide web to AI: 11 technology milestones that changed our lives

The world wide web is a key technological milestone in the past 40 years. Image: Unsplash/Ales Nesetril
.chakra .wef-1c7l3mo{-webkit-transition:all 0.15s ease-out;transition:all 0.15s ease-out;cursor:pointer;-webkit-text-decoration:none;text-decoration:none;outline:none;color:inherit;}.chakra .wef-1c7l3mo:hover,.chakra .wef-1c7l3mo[data-hover]{-webkit-text-decoration:underline;text-decoration:underline;}.chakra .wef-1c7l3mo:focus,.chakra .wef-1c7l3mo[data-focus]{box-shadow:0 0 0 3px rgba(168,203,251,0.5);} Stephen Holroyd
.chakra .wef-9dduvl{margin-top:16px;margin-bottom:16px;line-height:1.388;font-size:1.25rem;}@media screen and (min-width:56.5rem){.chakra .wef-9dduvl{font-size:1.125rem;}} Explore and monitor how .chakra .wef-15eoq1r{margin-top:16px;margin-bottom:16px;line-height:1.388;font-size:1.25rem;color:#F7DB5E;}@media screen and (min-width:56.5rem){.chakra .wef-15eoq1r{font-size:1.125rem;}} Artificial Intelligence is affecting economies, industries and global issues

.chakra .wef-1nk5u5d{margin-top:16px;margin-bottom:16px;line-height:1.388;color:#2846F8;font-size:1.25rem;}@media screen and (min-width:56.5rem){.chakra .wef-1nk5u5d{font-size:1.125rem;}} Get involved with our crowdsourced digital platform to deliver impact at scale
Stay up to date:, emerging technologies.
- It’s been 40 years since the launch of the Apple Macintosh personal computer.
- Since then, technological innovation has accelerated – here are some of the most notable tech milestones over the past four decades.
- The World Economic Forum’s EDISON Alliance aims to digitally connect 1 billion people to essential services like healthcare, education and finance by 2025.
On 24 January 1984, Apple unveiled the Macintosh 128K and changed the face of personal computers forever.
Steve Jobs’ compact, user-friendly computer introduced the graphical user interface to the world, marking a pivotal moment in the evolution of personal technology.
Since that day, the rate of technological innovation has exploded, with developments in computing, communication, connectivity and machine learning expanding at an astonishing rate.
Here are some of the key technological milestones that have changed our lives over the past 40 years.
Have you read?
9 ways ai is helping tackle climate change, driving trust: paving the road for autonomous vehicles, these are the top 10 emerging technologies of 2023: here's how they can impact the world, 1993: the world wide web.
Although the internet’s official birthday is often debated, it was the invention of the world wide web that drove the democratization of information access and shaped the modern internet we use today.
Created by British scientist Tim Berners-Lee, the World Wide Web was launched to the public in 1993 and brought with it the dawn of online communication, e-commerce and the beginning of the digital economy.
Despite the enormous progress since its invention, 2.6 billion people still lack internet access and global digital inclusion is considered a priority. The World Economic Forum’s EDISON Alliance aims to bridge this gap and digitally connect 1 billion people to essential services like healthcare, education and finance by 2025.
1997: Wi-Fi
The emergence of publicly available Wi-Fi in 1997 changed the face of internet access – removing the need to tether to a network via a cable. Without Wi-Fi, the smartphone and the ever-present internet connection we’ve come to rely on, wouldn’t have been possible, and it has become an indispensable part of our modern, connected world.
1998: Google
The launch of Google’s search engine in 1998 marked the beginning of efficient web search, transforming how people across the globe accessed and navigated online information . Today, there are many others to choose from – Bing, Yahoo!, Baidu – but Google remains the world’s most-used search engine.
2004: Social media
Over the past two decades, the rise of social media and social networking has dominated our connected lives. In 2004, MySpace became the first social media site to reach one million monthly active users. Since then, platforms like Facebook, Instagram and TikTok have reshaped communication and social interaction , nurturing global connectivity and information sharing on an enormous scale, albeit not without controversy .

2007: The iPhone
More than a decade after the first smartphone had been introduced, the iPhone redefined mobile technology by combining a phone, music player, camera and internet communicator in one sleek device. It set new standards for smartphones and ultimately accelerated the explosion of smartphone usage we see across the planet today.
2009: Bitcoin
The foundations for modern digital payments were laid in the late 1950s with the introduction of the first credit and debit cards, but it was the invention of Bitcoin in 2009 that set the stage for a new era of secure digital transactions. The first decentralized cryptocurrency, Bitcoin introduced a new form of digital payment system that operates independently of traditional banking systems. Its underlying technology, blockchain, revolutionized the concept of digital transactions by providing a secure, transparent, and decentralized method for peer-to-peer payments. Bitcoin has not only influenced the development of other cryptocurrencies but has also sparked discussions about the future of money in the digital age.
2014: Virtual reality
2014 was a pivotal year in the development of virtual reality (VR) for commercial applications. Facebook acquired the Oculus VR company for $2 billion and kickstarted a drive for high-quality VR experiences to be made accessible to consumers. Samsung and Sony also announced VR products, and Google released the now discontinued Cardboard – a low-cost, do-it-yourself viewer for smartphones. The first batch of Oculus Rift headsets began shipping to consumers in 2016.
2015: Autonomous vehicles
Autonomous vehicles have gone from science fiction to science fact in the past two decades, and predictions suggest that almost two-thirds of registered passenger cars worldwide will feature partly-assisted driving and steering by 2025 . In 2015, the introduction of Tesla’s Autopilot brought autonomous features to consumer vehicles, contributing to the mainstream adoption of self-driving technology.

2019: Quantum computing
A significant moment in the history of quantum computing was achieved in October 2019 when Google’s Sycamore processor demonstrated “quantum supremacy” by solving a complex problem faster than the world’s most powerful supercomputers. Quantum technologies can be used in a variety of applications and offer transformative impacts across industries. The World Economic Forum’s Quantum Economy Blueprint provides a framework for value-led, democratic access to quantum resources to help ensure an equitable global distribution and avoid a quantum divide.
2020: The COVID-19 pandemic
The COVID-19 pandemic accelerated digital transformation on an unprecedented scale . With almost every aspect of human life impacted by the spread of the virus – from communicating with loved ones to how and where we work – the rate of innovation and uptake of technology across the globe emphasized the importance of remote work, video conferencing, telemedicine and e-commerce in our daily lives.
In response to the uncertainties surrounding generative AI and the need for robust AI governance frameworks to ensure responsible and beneficial outcomes for all, the Forum’s Centre for the Fourth Industrial Revolution (C4IR) has launched the AI Governance Alliance .
The Alliance will unite industry leaders, governments, academic institutions, and civil society organizations to champion responsible global design and release of transparent and inclusive AI systems.
2022: Artificial intelligence
Artificial intelligence (AI) technology has been around for some time and AI-powered consumer electronics, from smart home devices to personalized assistants, have become commonplace. However, the emergence of mainstream applications of generative AI has dominated the sector in recent years.
In 2022, OpenAI unveiled its chatbot, ChatGPT. Within a week, it had gained over one million users and become the fastest-growing consumer app in history . In the same year, DALL-E 2, a text-to-image generative AI tool, also launched.
Don't miss any update on this topic
Create a free account and access your personalized content collection with our latest publications and analyses.
License and Republishing
World Economic Forum articles may be republished in accordance with the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Public License, and in accordance with our Terms of Use.
The views expressed in this article are those of the author alone and not the World Economic Forum.
Related topics:
The agenda .chakra .wef-n7bacu{margin-top:16px;margin-bottom:16px;line-height:1.388;font-weight:400;} weekly.
A weekly update of the most important issues driving the global agenda
.chakra .wef-1dtnjt5{display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;} More on Emerging Technologies .chakra .wef-17xejub{-webkit-flex:1;-ms-flex:1;flex:1;justify-self:stretch;-webkit-align-self:stretch;-ms-flex-item-align:stretch;align-self:stretch;} .chakra .wef-nr1rr4{display:-webkit-inline-box;display:-webkit-inline-flex;display:-ms-inline-flexbox;display:inline-flex;white-space:normal;vertical-align:middle;text-transform:uppercase;font-size:0.75rem;border-radius:0.25rem;font-weight:700;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;line-height:1.2;-webkit-letter-spacing:1.25px;-moz-letter-spacing:1.25px;-ms-letter-spacing:1.25px;letter-spacing:1.25px;background:none;padding:0px;color:#B3B3B3;-webkit-box-decoration-break:clone;box-decoration-break:clone;-webkit-box-decoration-break:clone;}@media screen and (min-width:37.5rem){.chakra .wef-nr1rr4{font-size:0.875rem;}}@media screen and (min-width:56.5rem){.chakra .wef-nr1rr4{font-size:1rem;}} See all

Nations target AI disinformation ahead of elections, and other digital technology stories you need to know
March 12, 2024

How universities can use blockchain to transform research
Scott Doughman

How Earth observation from space helps advance climate change research
Andrea Willige
March 6, 2024

How technology is driving net zero in the Middle East
Hatem Dowidar
March 5, 2024

The WTO extended a moratorium on digital trade tariffs. Here's why it will help innovation and productivity
Michele Ruta, Tibor Hanappi and Adam Jakubik
March 4, 2024

How can we secure AI in the era of infinite information?
Grant Bourzikas

COVID-19 vaccines: CDC says people ages 65 and up should get a shot this spring – a geriatrician explains why it’s vitally important
In my mind, the spring season will always be associated with COVID-19.
In spring 2020, the federal government declared a nationwide emergency , and life drastically changed. Schools and businesses closed, and masks and social distancing were mandated across much of the nation.
In spring 2021, after the vaccine rollout, the Centers for Disease Control and Prevention said those who were fully vaccinated against COVID-19 could safely gather with others who were vaccinated without masks or social distancing.
In spring 2022, with the increased rates of vaccination across the U.S., the universal indoor mask mandate came to an end.
In spring 2023, the federal declaration of COVID-19 as a public health emergency ended .
Now, as spring 2024 fast approaches, the CDC reminds Americans that even though the public health emergency is over, the risks associated with COVID-19 are not. But those risks are higher in some groups than others. Therefore, the agency recommends that adults age 65 and older receive an additional COVID-19 vaccine , which is updated to protect against a recently dominant variant and is effective against the current dominant strain.
Increased age means increased risk
The shot is covered by Medicare . But do you really need yet another COVID-19 shot?
As a geriatrician who exclusively cares for people over 65 years of age, this is a question I’ve been asked many times over the past few years.
In early 2024, the short answer is yes.
Compared with other age groups, older adults have the worst outcomes with a COVID-19 infection. Increased age is, simply put, a major risk factor .
In January 2024, the average death rate from COVID-19 for all ages was just under 3 in 100,000 people . But for those ages 65 to 74, it was higher – about 5 for every 100,000. And for people 75 and older, the rate jumped to nearly 30 in 100,000.
Even now, four years after the start of the pandemic, people 65 years old and up are about twice as likely to die from COVID-19 than the rest of the population. People 75 years old and up are 10 times more likely to die from COVID-19.
Vaccination is still essential
These numbers are scary. But the No. 1 action people can take to decrease their risk is to get vaccinated and keep up to date on vaccinations to ensure top immune response. Being appropriately vaccinated is as critical in 2024 as it was in 2021 to help prevent infection, hospitalization and death from COVID-19.
The updated COVID-19 vaccine has been shown to be safe and effective , with the benefits of vaccination continuing to outweigh the potential risks of infection .
The CDC has been observing side effects on the more than 230 million Americans who are considered fully vaccinated with what it calls the “ most intense safety monitoring in U.S. history .” Common side effects soon after receiving the vaccine include discomfort at the injection site, transient muscle or joint aches, and fever.
These symptoms can be alleviated with over-the-counter pain medicines or a cold compress to the site after receiving the vaccine. Side effects are less likely if you are well hydrated when you get your vaccine.
Long COVID and your immune system
Repeat infections carry increased risk, not just from the infection itself, but also for developing long COVID as well as other illnesses . Recent evidence shows that even mild to moderate COVID-19 infection can negatively affect cognition, with changes similar to seven years of brain aging. But being up to date with COVID-19 immunization has a fourfold decrease in risk of developing long COVID symptoms if you do get infected.
Read more: Mounting research shows that COVID-19 leaves its mark on the brain, including with significant drops in IQ scores
Known as immunosenescence , this puts people at higher risk of infection, including severe infection, and decreased ability to maintain immune response to vaccination as they get older. The older one gets – over 75, or over 65 with other medical conditions – the more immunosenescence takes effect.
All this is why, if you’re in this age group, even if you received your last COVID-19 vaccine in fall 2023, the spring 2024 shot is still essential to boost your immune system so it can act quickly if you are exposed to the virus.
The bottom line: If you’re 65 or older, it’s time for another COVID-19 shot.
- COVID-19 rapid tests still work against new variants – researchers keep ‘testing the tests,’ and they pass
- Mounting research shows that COVID-19 leaves its mark on the brain, including with significant drops in IQ scores
Laurie Archbald-Pannone receives funding from PRIME, Accredited provider of medical and professional education; supported by an independent educational grant from GlaxoSmithKline, LLC as Course Director "Advancing Patient Engagement to Protect Aging Adults from Vaccine-Preventable Diseases: An Implementation Science Initiative to Activate and Sustain Participation in Recommended Vaccinations”

- Share full article
Advertisement
Supported by
Guest Essay
‘Oppenheimer,’ My Uncle and the Secrets America Still Doesn’t Like to Tell

By Ariel Kaminer
Ms. Kaminer is an editor at Times Opinion.
The darkened sky stretches over miles of desert sand as in the distance, from an illuminated scaffold, the object rises that will change the world. The first atomic test is the defining scene in “Oppenheimer,” which won seven Academy Awards on Sunday night, including best picture. The scene plays out over seven or so minutes of steadily escalating tension: No one knew whether the bomb would go off at all that night and, if it did, whether it would incinerate the whole world.
Watching the film on opening weekend, I found the scene excruciating, even though history had long since recorded the outcome. I just kept staring at the Los Alamos scientists who gathered to witness the big event, lying under the stars as though taking in an outdoor movie, with nothing more to protect them than a small eye shade. The physicist Edward Teller is the only one who seems to recognize the need for any precautions, and he addresses it by applying sunscreen.
“Oppenheimer” is a movie about a singular genius, an extraordinary collaboration and a turning point in history. But it’s also a lesson in applied physics: the way a lone catalyst may trigger a chain reaction whose impact cannot be predicted or controlled. J. Robert Oppenheimer’s greatest triumph set into motion forces that brought about his downfall. An innovation designed to make the world safer in the long term made it manifestly more dangerous . And in subsequent atomic tests through the postwar years, many Americans were deliberately exposed to radiation, to see what the blast and its aftermath would do to them.
Soldiers were marched through detonation sites when the sand cooled down enough to walk on; pilots were sent through the still-billowing clouds; sailors were lined up on nearby boats. At the Yucca Flat testing grounds in Nevada, an Army band was even summoned to play. I know that last part because my uncle Richard Gigger was the band’s leader.
Richard enlisted in 1946. He was a 16-year-old Black kid in a still-segregated Army, but it got him from East St. Louis to Germany. While there, he got permission to attend a music training program in Dachau, of all places, led by members of the Berlin Philharmonic. It changed his life. Over the next decades he performed for heads of state, led ticker-tape parades through Manhattan and made numerous appearances on “The Ed Sullivan Show.”
On multiple occasions between 1952 and 1955, his responsibilities also included playing “Shake, Rattle and Roll” to accompany the most destructive force in human history.
Other atomic veterans , as they have come to be known, were in the South Pacific, wading through radioactive water while filling in blast craters. You can hear former service members speak about a range of these experiences — with pride, honor and a deep sense of betrayal — in a documentary called “ I Have Seen the Dragon .” Richard’s in it, too.
After 25 years spanning three wars, he retired from the Army and met my aunt Ellen. Together they started teaching music at San Fernando High School, where they led the marching band to so many championships — 13 in all, 11 of them consecutively — that it almost wasn’t fair. Along the way they mentored hundreds or maybe thousands of kids, many of whom still credit them with changing their lives. A school building and an intersection were renamed in tribute. There’s a huge mural , too. But eventually Richard’s military service caught up with him, as it did for so many others.
For Richard it started with a pituitary tumor. Surgeons removed it, but the result, a few years later, was a cranial bleed and brain damage that worsened over time.
As a kid I found my uncle kind but intimidating, a larger-than-life mix of showman’s bravado and military rigor. After the bleed, all that was gone. He moved slowly and said little. He could still play musical instruments, but in the documentary, it’s my aunt who speaks. Richard sits, silent. He died three months later.
For five decades, atomic veterans were forbidden to tell anyone about their experience, not even a spouse or doctor. That has made it hard to get a reliable accounting of their numbers, or of the medical consequences they suffered, which include leukemia, thyroid cancer, esophagus cancer and multiple myeloma. It has also made it hard for them or their family members to get needed support. To prove her case to the Department of Veterans Affairs, my aunt spent long hours in the library reading scientific articles about atmospheric ionizing radiation (many of which she first had to get translated from Japanese), went digging through the archives of old Nevada newspapers, consulted doctors. She was rebuffed many times but finally, after seven years, the V.A. relented. It confirmed that Richard’s condition was most likely caused by his exposure. That qualified her to receive modest compensation.
A number of conditions are now “ presumptive ” for atomic vets, meaning that they’re assumed to be a result of their service. But there’s no way to know how many people suffered or died before that policy was adopted or how many other conditions may also be the result of exposure — nor how many families couldn’t undertake the kind of research my aunt did or persevere through so many setbacks. The veterans’ numbers are dwindling, but these questions remain urgent, since the effects of radiation can be passed on to children and grandchildren.
“Oppenheimer” has been criticized for not showing the devastation in Hiroshima and Nagasaki. I think it was the right choice. It would have been offensive, maybe even obscene, to reduce that suffering to a subplot of a great-man biopic, a movie that, however deeply based in fact , is ultimately an entertainment, a fiction. Leaving Japan’s horror to the imagination, or to the intrusive thoughts you can see Oppenheimer struggling to shut out, felt to me like appropriate humility about the limits of representation, as when the film goes all but silent when the blast first registers.
As for the bomb’s effect on American bodies, the sight of those unprotected scientists is the closest the film comes. The scene plays like a metaphor for how naïvely optimistic the nuclear program was, how unprepared the nation, or even the world, was for the terrors it would unleash. After the test, when the Army guys crate up the remaining bombs and drive them away, Oppenheimer tells Teller, “Once it’s used, nuclear war, perhaps all war, becomes unthinkable.” Equally unthinkable, I suspect, would have been the idea that the United States would intentionally inflict some of the bomb’s harmful effects on its own service members.
If “Oppenheimer” were a more traditional film, Japan’s surrender might have been the climax. But the movie continues for another hour, turning its attention to Oppenheimer’s struggle to retain his security clearance, a fight that plays out in parallel with a Washington insider’s struggle to secure a cabinet post. It’s possible to leave the theater with the impression that, in the United States at least, the main victim of the bomb was Oppenheimer’s career.
For my uncle, the fallout came later. For some other atomic vets or their families — or for people living near test sites such as those in Nevada and the Marshall Islands and of course for people in Japan — it may yet be in the future. The film honored at the Oscars told a very specific story, but countless other lives trace back to that day, too. In one way or another, no one emerged untouched. We are all living downwind of that first momentous blast.
Ariel Kaminer is an editor at Times Opinion.
The Times is committed to publishing a diversity of letters to the editor. We’d like to hear what you think about this or any of our articles. Here are some tips . And here’s our email: [email protected] .
Follow the New York Times Opinion section on Facebook , Instagram , TikTok , X and Threads .
COMMENTS
The COVID-19 pandemic caused increased anxiety, depression, and other mental health concerns that were difficult for my family and me to manage alone. Our ability to learn social resilience skills, such as self-management, was tested numerous times. One of the most visible challenges we faced was social isolation and loneliness.
From lifestyle changes to better eating habits, people are using this time to get healthier in many areas. Since the pandemic started, nearly two-thirds of the survey's participants (62%) say ...
The days dragged on in my apartment, in black and white, like my photos. Sometimes we tried to smile, imagining that I was asymptomatic, because I was the virus. Our smiles seemed to bring good ...
It has been four years since the World Health Organization declared Covid-19 a global pandemic on March 11, 2020. ... In my past life, I'd have to be on the train in 15 minutes," said Ms ...
May 18, 2021 12:35 PM EDT. Connie Schultz is a Pulitzer Prize-winning columnist and the author of The Daughters of Erietown. E ight days after I was fully vaccinated, I boarded my first flight in ...
A World of Change. The changes and uncertainty brought on by the COVID-19 pandemic upset the order of many people's lives. But for Rachel Meyer, the director of community engagement for the Duke Divinity School's Theology, Medicine and Culture Initiative, the past two years have seen so much in her life fall into place.
Available in: English. ქართული. 12 May 2020. Being a school student can sometimes be challenging, but the COVID-19 pandemic has made getting an education, and life in general, even more difficult for young people in Georgia. With schools closed, lessons are being held remotely. All sports, school activities, and events have been ...
As we adapted to a new way of life, a study published in September 2021 in PLOS One found that people who experienced involuntary social role disruptions because of COVID-19 reported increased ...
Melva James, 42, is a cybersecurity consultant who grew up in Jackson, Miss., and lives in Massachusetts. The tumult of the past year inspired a dramatic life change. One of my best friend's ...
Alex, a writer and fellow disabled parent, found the freedom to explore a fuller version of herself in the privacy the pandemic provided. "The way I dress, the way I love, and the way I carry ...
Spring was an exceedingly challenging time because it wasn't only the COVID-19 context, but it was the murder of George Floyd. A lot of the students in my classes were out there in the streets protesting for social justice. In week nine or 10, one of the students turned on the camera and said, "The National Guard is right outside my window.
The outbreak has dramatically changed Americans' lives and relationships over the past year. We asked people to tell us about their experiences - good and bad - in living through this moment in history. Pew Research Center has been asking survey questions over the past year about Americans' views and reactions to the COVID-19 pandemic.
Writing About Coronavirus in Main and Supplemental Essays. Students can choose to write a full-length college essay on the coronavirus or summarize their experience in a shorter form. To help ...
By: Angela Murillo Martinez. It is no surprise that nobody's life is the same as it was before the pandemic occurred. Whether a student or a professor, or working at an office, or at a store, life has changed. As the number of cases in Travis and Williamson County continues to rise, life will continue to be different and will never be the same.
My content explains what my life was like during the last seven months of the Covid-19 pandemic and how it affected my life both positively and negatively. It also explains what it was like when I graduated from High School and how I want the future generations to remember the Class of 2020. Class assignment, Western Civilization (Dr. Marino).
How 2020 and covid-19 changed my life. Usually people like the New Year not only because they expect something unusual and great to happen during holidays, but also they hope that the coming year is going to bring a lot of positive changes to their lives and that they will gain new opportunities for self- realization, will have new contacts and ...
Melissa Blanco Dr Marino Western Civ. 9/18/20 My Life Experience During the Covid-19 Pandemic. In March of 2020, the entire world completely changed when the Coronavirus pandemic hit. In the last seven months, we have all been staying at home, wearing masks in public places, and trying to stay at least six feet away from other people in order ...
Ijuka Agnes Barongo. My life view changed just before Christmas when I got COVID-19. I was utterly shocked and kept asking how I could fail at observing the prevention protocols. Now I truly understand the psychological and physical meaning of living with COVID19. Not everyone is fortunate to have ready access to social services, so I am ...
1. Introduction. The coronavirus disease 2019 (COVID-19) pandemic has led to unprecedented changes in people's daily lives, with implications for mental health and well-being [1-4], both at the level of a given country's population, and when considering specific vulnerable groups [5-7].In order to mitigate the untoward impact of the pandemic (including lockdown) and support mental health ...
COVID-19 (Coronavirus) has affected day to day life and is slowing down the global economy. This pandemic has affected thousands of peoples, who are either sick or are being killed due to the spread of this disease. The most common symptoms of this viral infection are fever, cold, cough, bone pain and breathing problems, and ultimately leading ...
6. COVID-19 has already changed science immensely, but if scientists are savvy, the most profound pivot is still to come—a grand reimagining of what medicine should be. In 1848, the Prussian ...
Introduction. In December 2021, after many months of living with the COVID-19 pandemic, the world is still looking for a way out of this healthcare crisis. As of this writing, more than 250 million people globally have been infected with SARS-CoV-2, the virus that causes coronavirus disease 19 (COVID-19), and nearly 5 million individuals lost ...
This essay examines key aspects of social relationships that were disrupted by the COVID-19 pandemic. It focuses explicitly on relational mechanisms of health and brings together theory and emerging evidence on the effects of the COVID-19 pandemic to make recommendations for future public health policy and recovery. We first provide an overview of the pandemic in the UK context, outlining the ...
Reading time: 3 min (864 words) The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents an unprecedented challenge to public health, food systems and the world of work. The economic and social disruption caused by the pandemic is devastating: tens of millions of people are at risk of falling into extreme poverty ...
A new Lancet study reported the average life expectancy globally dropped by 1.6 years during the pandemic′s first two years. Among high-income nations, the U.S. fared especially poorly, with the highest excess mortality rate in 2020 and 2021. ... COVID-19 can change quickly from a distant news story to a battle for survival," the 2020 ...
The COVID-19 pandemic accelerated digital transformation on an unprecedented scale. With almost every aspect of human life impacted by the spread of the virus - from communicating with loved ones to how and where we work - the rate of innovation and uptake of technology across the globe emphasized the importance of remote work, video ...
In my mind, the spring season will always be associated with COVID-19. In spring 2020, the federal government declared a nationwide emergency, and life drastically changed. Schools and businesses ...
On the other hand, I was having these thoughts while watching "Past Lives" in a movie theater sitting next to my boyfriend, who is white. As an Asian woman living in the West, I learned long ...
People who test positive for Covid-19 no longer need to routinely stay away from others for at least five days, according to new guidelines from the US Centers for Disease Control and Prevention.
It changed his life. Over the next decades he performed for heads of state, led ticker-tape parades through Manhattan and made numerous appearances on "The Ed Sullivan Show."